
by top100admin | Jun 3, 2026 | AIMEDENT Journal Vol 1:4
As artificial intelligence reshapes clinical practice, one physician-executive argues that the real transformation is not technological — it is moral.
By Traci A. Kimball, MD, MBA
Physician Executive and Founder, The WISH Clinic® and Ekagra Health AI™
Every Patient Is Wounded Twice
Every patient who walks into my wound care clinic arrives with two injuries. The first is physical — a chronic wound that may have resisted treatment for months or years. The second is systemic: a deep, persistent loss of faith that the healthcare system is capable of healing them at all.
I became a wound care physician because I believed I could address both. Over decades of practice, I learned that the act of healing is never purely clinical. It is relational, spiritual even — a covenant between a suffering person and the professional who commits, without reservation, to walking with them until the wound closes or every ethical option has been exhausted. My mother called it simply: if you love your work, it is not work. I call it the laying on of hands.
Now, a new companion has joined us on that journey. Artificial intelligence is entering the exam room, the operating suite, and the billing department simultaneously. And the central question facing every physician, health system leader, and technology executive at this conference is not whether AI will transform medicine. It already is. The question is whether we will allow it to make medicine colder — or more human.
Three Eras, One Reckoning
To understand where we are going, we must reckon honestly with where we have been. Wound care — and medicine more broadly — has passed through three distinct eras in my lifetime.
Woundcare 1.0 was the humanist era. Bedside medicine. The physician as healer, diagnostician, and companion. Empathy was not a soft skill; it was the primary instrument of care. Bureaucracy was minimal. Trust was the currency of the clinical relationship.
Woundcare 2.0 arrived as the fee-for-service era consolidated its grip on American healthcare. Volume replaced value. Data replaced discernment. Physicians became documentation engines, their clinical time consumed by EHR fields that generated revenue but rarely improved outcomes. The wound care specialist who once spent forty-five minutes with a complex patient now had twelve. The system did not break physicians’ desire to heal. It simply starved it of oxygen.
Woundcare 3.0 is the era we are now entering — and it is, I believe, our last best opportunity to restore what was lost. Artificial intelligence, deployed with intention and governed by ethics, can return to the physician what the administrative burden stole: time, attention, and the cognitive space required for genuine clinical presence.
“AI must learn bedside manner before it learns billing codes.”
The Co-Pilot, Not the Replacement
At Ekagra Health, the AI platform I co-founded, we designed our system around a single governing principle: the physician is not a problem to be automated away. The physician is the point.
Our platform integrates EHR management, revenue cycle automation, real-time outcomes analytics, laboratory workflow, patient communications, and compliance infrastructure into a unified intelligence layer. But the architecture of that system reflects a deliberate moral choice. Every module was built to reduce the friction that pulls clinicians away from patients — not to replace the judgment that draws them toward them.
When AI absorbs the complexity of prior authorizations, denial management, and documentation, something remarkable happens: physicians remember why they went to medical school. They look up from their screens. They ask the question that the algorithm cannot yet ask, because it requires the full weight of human presence to ask it well: How are you, really?
This is not sentimentality. It is clinical strategy. Research consistently demonstrates that patient engagement, therapeutic alliance, and perceived empathy are among the strongest predictors of treatment adherence and wound healing outcomes. A physician restored to presence is a more effective physician. AI that serves that restoration is not merely efficient — it is therapeutic.
Leading Change, Not Just Adopting Technology
The implementation of AI in healthcare is, at its core, a leadership problem disguised as a technology problem. I have learned this the hard way.
For years, I believed that leading change meant having the answer first — arriving at the M&M conference with the diagnosis already formed, the solution already sketched. What my own leadership development revealed, uncomfortably, was that this instinct was not strength. It was a form of control that crowded out collaboration, silenced nurses who had seen what I had not seen, and made the team smaller than it needed to be.
The transformation I underwent — from the physician who needed to be the smartest person in the room to the leader who understood that the room itself is the intelligence — maps directly onto the challenge facing health systems today. Organizations that deploy AI as a top-down efficiency mandate will reap resistance, workarounds, and moral injury. Organizations that deploy it as an act of collaborative leadership — inviting clinicians into the design, celebrating early adopters, embedding new workflows slowly and with care — will reap culture change that lasts.
Kotter’s foundational insight remains true in the age of machine learning: change does not succeed because technology exists. It succeeds because people are ready. And people become ready when they are treated not as users to be onboarded, but as healers to be honored.
A New Oath for a New Era
At medical school graduation, we pledged to do no harm. The Hippocratic tradition asked us to hold the patient’s welfare above our own convenience, our own profit, our own pride. It was a moral framework sufficient for a world in which the physician was the most powerful actor in the clinical encounter.
That world no longer exists. Today, the algorithm is also present in the exam room. The insurance adjudication engine is present. The EHR vendor’s incentive structure is present. The venture capital thesis that underwrites the AI platform is present. Medicine has never been a more crowded moral space.
Which is why I would propose, for every technologist, executive, and clinical leader gathered at this conference, a supplementary oath: do no hubris.
Do not assume that because an algorithm performs better than a physician on a diagnostic benchmark, it is ready to be a physician. Do not assume that because a machine can predict wound deterioration with 94% sensitivity, it understands what it means to a 74-year-old woman to lose her ability to walk. Do not assume that efficiency and healing are the same thing, or that speed and care are synonymous.
The greatest wound in healthcare today is not biological. It is systemic. It is the accumulated damage of decades in which the infrastructure of medicine — its incentives, its technology, its administrative architecture — was designed to extract value rather than create it. Healing that wound requires the same qualities we bring to the bedside: honesty about what is broken, courage to change it, and the humility to know we will not do it alone.
The road ahead is long. But for the first time in my career, I believe the technology exists to walk it well. The only question is whether we have the wisdom to let it serve our humanity — rather than replace it.
About the Author
 Traci A. Kimball, MD, MBA is a physician executive, wound care specialist, and the founder of The WISH Clinic® and Ekagra Health AI™. She will deliver the keynote address “From Wound Wizardry to Woundcare 3.0” at the Global Success Institute’s AI in Medicine Conference in June 2026. She writes and speaks on the intersection of clinical leadership, health technology, and the ethics of human-centered AI.
Traci A. Kimball, MD, MBA is a physician executive, wound care specialist, and the founder of The WISH Clinic® and Ekagra Health AI™. She will deliver the keynote address “From Wound Wizardry to Woundcare 3.0” at the Global Success Institute’s AI in Medicine Conference in June 2026. She writes and speaks on the intersection of clinical leadership, health technology, and the ethics of human-centered AI.

by top100admin | Jun 3, 2026 | AIMEDENT Journal Vol 1:3
Introduction: The wrong question
Artificial intelligence (AI) is rapidly transforming dental practice. From radiographic interpretation to risk prediction and treatment planning, AI systems are increasingly embedded within routine clinical workflows.
Yet, the dominant question often posed—whether AI will replace dentists—is ultimately misleading. The real transformation lies elsewhere. AI is not replacing dentists; it is reshaping the very nature of clinical responsibility.
The dentist of the future will not compete with machines but will work alongside them, navigating an increasingly complex decision-making environment where human judgement remains central.
From operator to decision-maker
Traditionally, dentistry has been grounded in technical skill supported by clinical judgement. Dentists examine, diagnose, and perform procedures based on experience and evidence.
Today, AI systems assist in detecting caries, identifying periodontal disease, analysing radiographs, and even simulating orthodontic outcomes. These tools do not replace clinical decision-making—but they increasingly influence it.
As a result, the clinician’s role is shifting from procedural execution to high-level interpretation. The dentist becomes a decision-maker within a technologically augmented system, where understanding context is as important as performing treatment.
The new responsibility: judging the machine
With AI integration comes a new responsibility: evaluating the reliability of algorithmic outputs.
Clinicians must now consider:
- The quality and completeness of input data
- The population on which the algorithm was trained
- The presence of bias or uncertainty
- Whether the recommendation aligns with clinical findings
This layer of judgement did not previously exist. It requires dentists to critically assess not only patients, but also the tools used to evaluate them.
The risk of automation bias
Automation bias—the tendency to over-trust machine outputs—is a growing concern in AI-supported healthcare.
In dental practice, even subtle visual cues, such as highlighted lesions on radiographs, can influence decision-making. Clinicians may unconsciously accept AI suggestions, particularly under time pressure.
This can lead to overtreatment, missed diagnoses, or reduced critical thinking. Ironically, the more accurate AI becomes, the greater the risk that clinicians may rely on it without sufficient scrutiny.
Clinical reality: where responsibility is tested
The true challenge of AI emerges in real clinical scenarios.
Consider a radiograph with slight artefacts. An AI system may still generate diagnostic probabilities. The clinician must determine whether these outputs are valid or misleading.
Similarly, implant planning systems may suggest optimal positioning based on digital simulations, yet fail to incorporate systemic health, patient behaviour, or surgical variability.
In each case, AI provides information—but responsibility for interpretation remains entirely with the clinician.
Redefining competence in the AI era
Competence in dentistry is evolving.
In addition to traditional clinical skills, dentists must now:
- Understand how AI systems function
- Recognise their limitations
- Identify uncertainty and bias
- Communicate AI-assisted decisions transparently
This does not require deep technical expertise, but it does require a new form of literacy—AI literacy. Without it, clinicians risk misinterpreting or over-relying on algorithmic outputs.
Designing safer AI systems
Responsibility must also be embedded within AI design.
Current systems prioritise accuracy but often lack mechanisms to communicate uncertainty. Future AI tools should:
- Indicate confidence levels
- Detect out-of-scope data
- Provide explainable outputs
- Encourage clinician oversight
The goal is not to create systems that always provide answers, but systems that recognise when they should remain uncertain or silent.
Ethics: responsibility cannot be delegated
At its core, the integration of AI raises an essential ethical question: who is responsible for patient outcomes?
Despite technological advancement, responsibility cannot be transferred to algorithms. The clinician remains accountable for diagnosis, treatment planning, and patient care.
This reflects fundamental ethical principles—beneficence, non-maleficence, autonomy, and justice—which remain unchanged in the digital age.
Conclusion: A profession redefined, not replaced
Artificial intelligence is not replacing dentists. It is redefining their role.
The future dentist will operate at the intersection of clinical expertise and technological insight. Success will depend not on how much AI is used, but on how effectively it is evaluated.
In this evolving landscape, clinical responsibility becomes the defining skill of modern dentistry. And ultimately, the responsibility for patient care will always remain human.
References
- Schwendicke F, Samek W, Krois J. Artificial intelligence in dentistry: chances and challenges. J Dent Res. 2020;99(7):769–774.
- Topol EJ. High-performance medicine: the convergence of human and artificial intelligence. Nat Med. 2019;25:44–56.
- Esteva A, et al. A guide to deep learning in healthcare. Nat Med. 2019;25:24–29.
- NHS England. Artificial Intelligence in Health and Care: Policy framework. 2023.
- World Health Organization. Ethics and Governance of Artificial Intelligence for Health. 2021.
About the author
 Dr. Ameed Khalid Abdul-Hamid is an Iraqi–British dental surgeon and academic researcher, internationally recognized for his contributions to artificial intelligence in dentistry and healthcare. He holds advanced qualifications from the University of Baghdad and the University of London, and is a Fellow of the Royal College of Surgeons (UK). Dr. Abdul-Hamid serves as Chairman of the Arab Organisation for Artificial Intelligence in Healthcare and Chairman of the Saudi-British Medical Forum (London). His research focuses on AI-enabled diagnostics, digital health systems, and the ethical, responsible integration of artificial intelligence in clinical care. In 2025, his work in dental artificial intelligence was published in the British Dental Journal, and he is a recipient of the Alan Turing Award in Dental Artificial Intelligence.
Dr. Ameed Khalid Abdul-Hamid is an Iraqi–British dental surgeon and academic researcher, internationally recognized for his contributions to artificial intelligence in dentistry and healthcare. He holds advanced qualifications from the University of Baghdad and the University of London, and is a Fellow of the Royal College of Surgeons (UK). Dr. Abdul-Hamid serves as Chairman of the Arab Organisation for Artificial Intelligence in Healthcare and Chairman of the Saudi-British Medical Forum (London). His research focuses on AI-enabled diagnostics, digital health systems, and the ethical, responsible integration of artificial intelligence in clinical care. In 2025, his work in dental artificial intelligence was published in the British Dental Journal, and he is a recipient of the Alan Turing Award in Dental Artificial Intelligence.

by top100admin | Jun 3, 2026 | AIMEDENT Journal Vol 1:3
For years, the conversation around AI in dentistry has focused on what the technology can detect, automate, or generate.
Can AI identify pathology on radiographs?
Can it automate notes?
Can it create treatment simulations?
Can it improve scheduling, billing, or recall systems?
These are meaningful advances. But they all share the same underlying assumption:
That dentistry’s primary bottleneck is producing more information.
It isn’t.
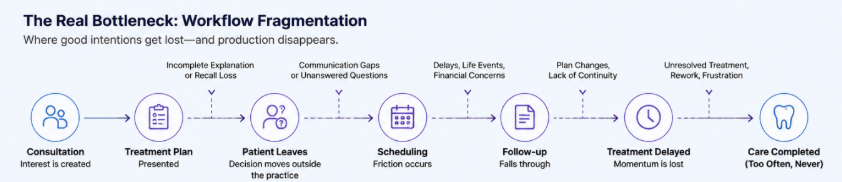
The real bottleneck is what happens to information after it is created.
In many workflows, fragmentation begins long before the patient leaves the clinic. Findings, explanations, treatment sequencing, documentation, communication, and follow-up systems often evolve separately instead of forming one continuous patient journey.
Across modern dental organizations, treatment plans are presented every day with clear clinical intent and genuine patient benefit. Yet enormous amounts of accepted treatment never become completed care. Patients delay. Follow-ups fragment. Explanations vary between providers. Documentation loses continuity. Teams spend more time recovering workflow breakdowns than preventing them.
The problem is no longer data scarcity. The problem is operational fragmentation.
The Industry Has Optimized Detection. It Has Not Optimized Continuity.
Modern practices already generate enormous amounts of clinical information:
- radiographs
- intraoral scans
- photographs
- periodontal charting
- SOAP notes
- treatment plans
- scheduling history
- communication logs
- financial records
But most of this information exists as disconnected fragments.
One system stores imaging.
Another stores notes.
Another manages communication.
Another tracks treatment acceptance.
Another tracks billing.
The result is that practices often have more data than ever — but less operational clarity.
This issue becomes especially visible in elective and comprehensive treatment workflows, where success depends not only on diagnosis, but on maintaining continuity across time.
A consultation may go extremely well. The patient is engaged. They ask questions. They appear motivated. The treatment plan makes clinical sense.
A patient may verbally accept treatment during consultation, but the workflow later fragments through delayed scheduling, unanswered questions, financing uncertainty, or inconsistent follow-up communication.
And the workflow begins to fragment.
The Decision Window Is Where Most Production Disappears
One of the most overlooked realities in dentistry is that treatment decisions are rarely finalized inside the consultation room.
They happen afterward:
- during the drive home
- in conversations with spouses or family
- while reviewing estimates later at night
- after financial anxiety appears
- after details are partially forgotten
- after confidence begins to decay
Research consistently shows that patients remember only a fraction of healthcare information after consultations. The more complex the treatment discussion, the greater the loss of recall.
This becomes highly relevant in esthetic, restorative, and multidisciplinary dentistry, where treatment acceptance depends heavily on understanding, confidence, perceived value, and emotional certainty — not merely diagnosis.
The industry has traditionally treated this as:
- a sales issue
- a financing issue
- a communication issue
But operationally, it is something else:
a continuity problem.
The consultation creates momentum but most workflows fail to preserve it.
Case Acceptance Is Not the Same as Case Completion
One of the most important operational insights emerging in modern dentistry is that accepted treatment does not necessarily become completed treatment.
A recent analysis of thousands of dental practices found that average case completion rates remain dramatically lower than treatment acceptance rates.
In other words:
Patients often say “yes” — but the workflow fails afterward.
This changes how we should think about operational performance.
The bottleneck is not only convincing patients to proceed. The bottleneck is maintaining continuity between:
- diagnosis
- explanation
- scheduling
- documentation
- follow-up
- long-term treatment progression
The highest-performing organizations are not simply presenting more treatment.
They are reducing workflow friction between clinical intent and completed care.
The Next Generation of AI Will Focus on Workflow Intelligence
Most current AI systems in dentistry optimize outputs:
- image interpretation
- note generation
- simulation rendering
- risk scoring
- scheduling automation
The next generation will optimize workflows. This is a fundamentally different layer of intelligence.
Why This Matters for DSOs and Large Organizations
As organizations scale, operational inconsistency compounds.
This creates hidden operational volatility.
Interestingly, recent DSO operational data suggests that consistency itself may be one of the strongest predictors of sustainable growth. Organizations with stable operational patterns significantly outperform highly volatile organizations.
The implication is important:
The future competitive advantage in dentistry may not come from who detects the most findings.
It may come from who operates with the most continuity.
From Static Records to Continuous Clinical Context
Historically, dental software systems were designed primarily as:
- scheduling tools
- billing systems
- documentation repositories
But modern clinical environments increasingly require something different.
This is where workflow intelligence becomes clinically and commercially relevant.
Because continuity is not only about efficiency.
It directly affects:
- patient trust
- treatment acceptance
- scheduling predictability
- provider stress
- documentation defensibility
- operational scalability
Dentistry’s Next AI Phase Will Be Less About Automation — And More About Coordination
The first wave of dental AI focused on assistance:
- helping clinicians detect
- summarize
- automate
- visualize
The next phase will focus on coordination:
- aligning teams
- preserving treatment understanding
- reducing workflow fragmentation
- improving operational predictability
- maintaining continuity across the patient journey
This is a more difficult problem than image detection.
But it is also a more consequential one because the practices and organizations that solve continuity effectively will not simply produce more dentistry.
They will create:
- more predictable operations
- more consistent patient experiences
- more complete treatment journeys
- and ultimately, more trusted healthcare systems
Importantly, solving continuity cannot depend on adding more administrative burden to clinicians already overwhelmed by documentation and workflow complexity.
The future of dental AI may not belong to the systems that generate the most information, but to the systems that help teams maintain clarity, continuity, and patient confidence from first consultation to completed care.
About the author
 Dr. Sami Savolainen is a dentist and founder of SmileMatch, a platform focused on clinical workflow intelligence, treatment communication, and documentation continuity. Combining clinical experience with system design, he explores how operational workflows influence treatment acceptance, patient trust, consistency, and scalability in modern healthcare.
Dr. Sami Savolainen is a dentist and founder of SmileMatch, a platform focused on clinical workflow intelligence, treatment communication, and documentation continuity. Combining clinical experience with system design, he explores how operational workflows influence treatment acceptance, patient trust, consistency, and scalability in modern healthcare.

by top100admin | Jun 2, 2026 | AIMEDENT Journal Vol 1:3
Human override remains essential, but it cannot protect patients if uncertain inputs have already been transformed into confident clinical conclusions.
— Dr. Naela Aldughmi
In dentistry, we are witnessing a significant shift in how artificial intelligence is being integrated into clinical practice. We are moving beyond single-task AI tools that flag isolated findings or assist with narrow tasks. We are entering the era of agentic AI: systems that can gather information, compare serial records, generate treatment options, draft clinical notes, and influence decisions more quietly than we realize.
This evolution brings exciting possibilities—better organization of patient data, clearer communication during consultations, more consistent documentation, and more efficient workflows. Yet it also introduces a new category of risk that deserves careful attention.
The danger is not AI assisting. The real risk begins when a system silently crosses from assisting to recommending to deciding—without showing the dentist the reasoning behind each step.
In my years practicing aesthetic and restorative dentistry, I have learned that the quality of any clinical decision depends heavily on the integrity of the information it is built upon. This principle becomes even more critical as AI systems grow more autonomous.
Dentistry’s Unique Vulnerability to Agentic AI
Dental and aesthetic decisions rest on a complex web of interdependent inputs. We evaluate faces in motion and at rest. We assess lip dynamics, tooth display, gingival architecture, occlusion, periodontal support, restorative space, tooth wear, facial balance, soft-tissue behavior, function, and patient expectations—often before deciding whether a concern is restorative, orthodontic, periodontal, surgical, aesthetic, or a combination of these.
A frontal smile photo, a 3D scan, or a single radiograph tells only part of the story. When these elements are combined poorly or interpreted too aggressively by AI, the output can look impressive while remaining clinically incomplete.
I have seen how polished digital outputs can mask basic capture problems: suboptimal lighting that changes the apparent tooth proportions, slight head rotation that affects perceived midline alignment, or lip strain that alters the impression of gingival display. In a busy practice, these details can easily be missed especially when the AI presents its result with clean visuals and confident language.
That is where agentic AI becomes different from a simple report. A passive system may state, “asymmetric smile noted.” A more agentic system may compare previous records, flag possible orthodontic or restorative discussion areas, estimate case complexity, and draft consultation language. Each step may be useful. Together, they can gradually shift control away from the clinician unless the system is built with clear safety boundaries.
Why Human Override at the End Is Not Enough
Many thoughtful voices in dental AI emphasize human judgment and clinician override. I agree completely. But override at the final stage is necessary; it is not a complete safety architecture.
By the time a confident treatment suggestion reaches the dentist’s screen, several quiet failures may already have occurred:
- Poor-quality or incomplete inputs accepted without warning
- Unstable landmarks used for measurements
- Proxy metrics presented with the authority of direct measurements
- Overconfident clinical language replacing cautious interpretation
- No clear audit trail showing what the AI suppressed, downgraded, or assumed
Workflow drift can happen easily. Staff may begin treating AI outputs as the default plan. Patients may arrive believing a sleek visualization represents a clinical recommendation. Without proper architecture, the dentist ends up reacting rather than directing.
Responsible AI in dentistry must therefore address safety earlier in the pipeline, not only at the final approval stage.
The Capture-to-Conclusion Safety Chain
This is the central idea I believe our profession should adopt before embracing greater AI autonomy. Every AI-generated output in dentistry should be traceable through a Capture-to-Conclusion Chain. The goal is not to slow innovation, but to make it trustworthy.
1. Capture
The first and most important gate is input quality. Before producing any confident output, the system should evaluate whether the captured data is clinically usable.
In practice, this means checking for frontal alignment, lighting, blur, facial rotation, natural smile position, excessive lip strain, complete tooth exposure, and correct orientation of 3D scans. If the patient was not looking straight ahead, or if lighting created harsh shadows, the system should not generate polished measurements or simulations as if the data were ideal. It should flag the limitation clearly and ask for better records.
A poor capture should never be allowed to produce an elegant conclusion. That early honesty protects both patient and clinician.
2. Calculation
Once acceptable data is captured, the system must be transparent about how it derives numbers and insights. It should clearly separate:
- Direct, calibrated measurements
- Calibrated estimates
- Proxy metrics
- Visual observations
- Unreliable or intentionally suppressed data
In clinical terms, a displayed “maxillary incisal display of 3.8 mm” carries very different weight depending on whether it came from a calibrated smile video with stable lip landmarks or from an extrapolated estimate on a single 2D photograph. Likewise, a tooth-width measurement from a properly oriented intraoral scan carries a different level of reliability than a visual estimate from a smile photo.
The dentist deserves to know which kind of measurement is being shown. Every important number should carry its provenance.
3. Conclusion
Finally, the system must maintain strict boundaries between observation, interpretation, discussion points, and actual clinical decisions. AI can organize findings, highlight patterns across records, and prepare options for discussion. But the final synthesis—the moment where data becomes a treatment plan—belongs to the dentist.
That synthesis must still include examination, radiographs where indicated, periodontal and occlusal assessment, functional risk, patient goals, medical history, and long-term maintenance considerations.
This clear separation prevents AI-generated text from quietly becoming the default clinical plan simply because it sounds professional and authoritative.
What Responsible Dental AI Should—and Should Not—Do
A well-designed system can become a valuable clinical partner by:
- Helping organize complex observations across multiple records
- Improving consultation clarity with visual aids that respect input limitations
- Standardizing documentation while preserving the dentist’s voice
- Highlighting measurable patterns and changes over time
- Showing confidence levels and downgrading when appropriate
- Refusing to generate outputs from weak inputs
- Maintaining a complete, reviewable audit trail
Equally important is knowing what good AI must refuse to do. It should not diagnose or suggest definitive treatment from insufficient data. It should not convert subjective aesthetic preferences into clinical “needs.” It should not present proxy metrics as precise measurements. It should not hide uncertainty behind smooth wording. And it should never replace hands-on examination, proper imaging protocols, or the dentist’s integrated judgment.
A Practical Checklist for Dentists
When evaluating AI tools for clinical use, dentists should ask:
- Does the system evaluate input quality before generating outputs?
- Can I see the provenance and confidence level of each measurement?
- Does it distinguish between observation, interpretation, and recommendation?
- Does it explain whether a result is calibrated, estimated, or only a proxy?
- If I repeat the capture, does the system give similar measurements?
- Is there a transparent audit trail I can review?
- Can I override or adjust any step in the chain?
- Does the system default to conservative language when data is limited?
Tools that answer “yes” to these questions are not merely producing attractive reports. They are building the kind of safety architecture dentistry needs.
Looking Ahead
The future of dental AI should not be a sophisticated black box that quietly moves from Assist to Decide. It should be a disciplined, transparent partner—one that shows its work clearly, knows its limits honestly, and keeps the dentist responsible for final clinical judgment.
By demanding proper Capture-to-Conclusion safety chains today, we protect patient safety, professional integrity, and the irreplaceable value of human clinical reasoning. Responsible innovation does not mean resisting progress. It means shaping progress so technology serves our patients and strengthens, rather than erodes, the human core of dentistry.
Author Bio
 Dr. Naela AlDughmi is a practicing aesthetic and restorative dentist based in Amman, Jordan. She is the founder of IrisAthena and writes on the responsible integration of technology into clinical dentistry.
Dr. Naela AlDughmi is a practicing aesthetic and restorative dentist based in Amman, Jordan. She is the founder of IrisAthena and writes on the responsible integration of technology into clinical dentistry.
by top100admin | Jun 1, 2026 | News
The crypto super app for trading, predicting, and earning. Buy 90+ cryptos, trade prediction markets, and earn with staking and the Gemini Credit Card.
