by top100admin | Jun 5, 2026 | AIMEDENT Journal Vol 1:4
In clinical AI, progress is easy to signal and difficult to achieve. A model is validated. A pilot launches. A press release announces state-of-the-art performance. From the outside, it looks like momentum. Inside the hospital, the clinician works within the same constraints, the workflow carries the same load, and the patient experiences no difference. The model exists; adoption does not. That distance, the space between what an algorithm can do in validation and what it changes in care, is the central economic fact of healthcare AI, and almost no one is pricing it correctly.
The evidence describes a field investing in capability and waiting on impact. According to Rock Health, U.S. digital health funding reached $14.2 billion in 2025, up 35% over the prior year, with companies centering AI capturing 54% of it, up from 37% a year earlier. Yet a 2025 McKinsey survey found that only about 39% of organizations report any enterprise-level earnings impact from AI, and most of that impact is under 5%. Capital is flowing toward model capability while the return on it lags. The constraint is rarely model quality; less than 60% of the data healthcare organizations already generate is used in decision-making. The capacity to build models has outrun the capacity to absorb them, and almost no one is pricing that gap correctly.
Why AI Widens the Distance
AI does not close the gap between science and care by default; in important ways it widens it. Predictive models are extrapolation engines: they describe risk well and rarely change it, because a probability is not an intervention. Convergence AI, the merging of once-separate fields (biology, imaging, language, and clinical data) into systems that reason across all of them at once, compounds discovery faster than any prior wave of healthcare technology, and faster than delivery systems can absorb. Generative medicine, in which AI designs novel therapeutics and interventions on demand rather than merely predicting risk, is the sharpest current expression of that acceleration. Each advance enlarges the same distance: capability races ahead, and adoption waits.
The failure is specific, not vague. Models that perform in validation degrade in live clinical settings: distribution shift as local populations diverge from training data, workflow mismatch when an output arrives at the wrong moment in care, alert fatigue that turns signal into noise, and an integration burden that no benchmark measures. The pattern is documented. A widely deployed proprietary sepsis prediction model, live in hundreds of U.S. hospitals, was found on external validation to identify only about a third of sepsis cases while generating enough false alerts to fatigue the clinicians it was meant to help (Wong et al., JAMA Internal Medicine, 2021). The tool was not absurd; it simply did not survive contact with a real ward. Dentistry shows the same shape: AI that reliably flags caries or bone loss on a radiograph still changes nothing if it arrives outside the moment the clinician decides on treatment. A model can be accurate and still go unused, and an unused model changes nothing.
The contrast proves the point. A different sepsis system, deployed across five hospitals and monitoring more than 590,000 patients, was studied prospectively and reported in Nature Medicine in 2022. Among septic patients whose alert a clinician confirmed within three hours, in hospital mortality fell by roughly 18% (Henry et al., Nature Medicine, 2022). What separated this result from the failures was not a more brilliant algorithm; it was that the system earned sustained clinician use, near 89%, by fitting the way care already moved. The benefit tracked the adoption, not merely the prediction. Same disease, two models, opposite outcomes, and the difference lived in everything around the model rather than in the model itself.
This is why benchmark performance has become a poor predictor of clinical impact, and why the hard problem in healthcare AI has migrated from the model to everything around it.
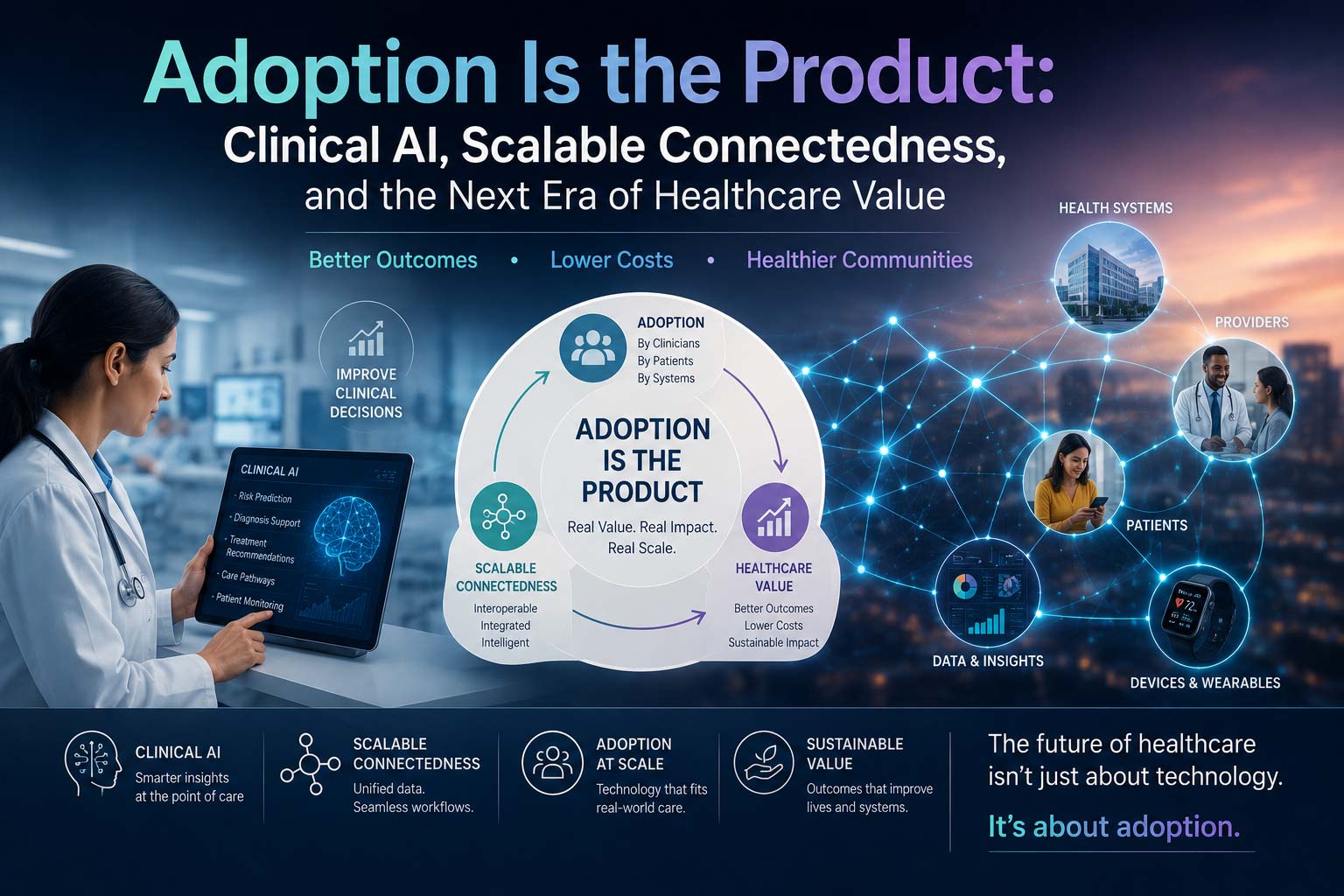
The Thesis: Scalable Connectedness
This is the space I have spent my career studying, and it is the foundation of how I invest. I call it scalable connectedness. The premise is simple: science is accelerating faster than accessibility, and AI is the accelerant. The distance between what a model can do and what reaches the people who need it is widening, not closing. Most treat that distance as a gap to be lamented. I treat it as among the most underpriced spaces in healthcare AI, because it is where category-defining companies are built. Durable value does not come from a better model. It comes from connecting model capability to clinical adoption at scale.
That reframing changes what a strong AI company looks like and what a disciplined investor should underwrite. The defensible asset is not the algorithm; algorithms are increasingly abundant and quickly matched. The defensible asset is the ability to carry a model across the last and hardest distance, into a workflow, a reimbursement pathway, a clinician’s daily habit, a patient’s actual life. In clinical AI, the product is not the model. The product is the behavior change the model makes possible inside the system.
The Adoption Test
If adoption is the product, then adoption is where diligence should concentrate. The question that predicts outcomes is not “is the model accurate?” Most models are accurate in a demo. Three questions matter more:
- What specific clinical behavior has to change for this model to be used?
- Who owns that change, and do they have the authority and the incentive to see it through?
- Once the change is made, is it durable, or does it reverse the moment attention moves elsewhere?
A team that can answer those three is solving the problem that actually separates the clinical-AI winners from the graveyard of accurate, well-funded models that no one adopted.
Three Audiences, One Direction
This thesis speaks differently to the three groups building healthcare AI, but it points them the same way. For those allocating capital, durable returns favor the work that moves a model into care (the integration, the workflow, the trust) over the one-time benchmark win that never travels. For founders, the most defensible position is the one closest to the patient: owning the distance between what a model can compute and what a clinician can act on. For physician innovators, the clinical vantage point is not a detour from the work. It is a design advantage, because knowing exactly where care breaks down is knowing exactly where a model can create value.
And it answers a question I am asked often: whether purpose and return are at odds. They are not. The companies that move AI from capability to bedside are, in the same motion, the ones that compound. Dignity delivered at scale and durable financial performance are not competing objectives in this field. They are one objective seen from two sides.
Conclusion
Healthcare’s next era will not be defined by who builds the most capable model. It will be defined by who connects model capability to the people it was meant to serve. That is an engineering problem, an investment problem, and, for those of us who came to this work from medicine, a moral one. The space between what AI can compute and what care can use is not empty. It is where the future of healthcare value will be built, by the founders and the funds willing to treat connectedness itself as the thing worth building.
About the author
 Mohammed Quadri, MD, MBA, is a physician Enterpreneur, investor, and healthcare strategist focused on clinical AI, biotech, and life sciences from innovation through adoption. His work centers on scalable connectedness: the principle that durable value comes from connecting invention to adoption at scale, where purpose and returns advance together.
Mohammed Quadri, MD, MBA, is a physician Enterpreneur, investor, and healthcare strategist focused on clinical AI, biotech, and life sciences from innovation through adoption. His work centers on scalable connectedness: the principle that durable value comes from connecting invention to adoption at scale, where purpose and returns advance together.
by top100admin | Jun 4, 2026 | AIMEDENT Journal Vol 1:3
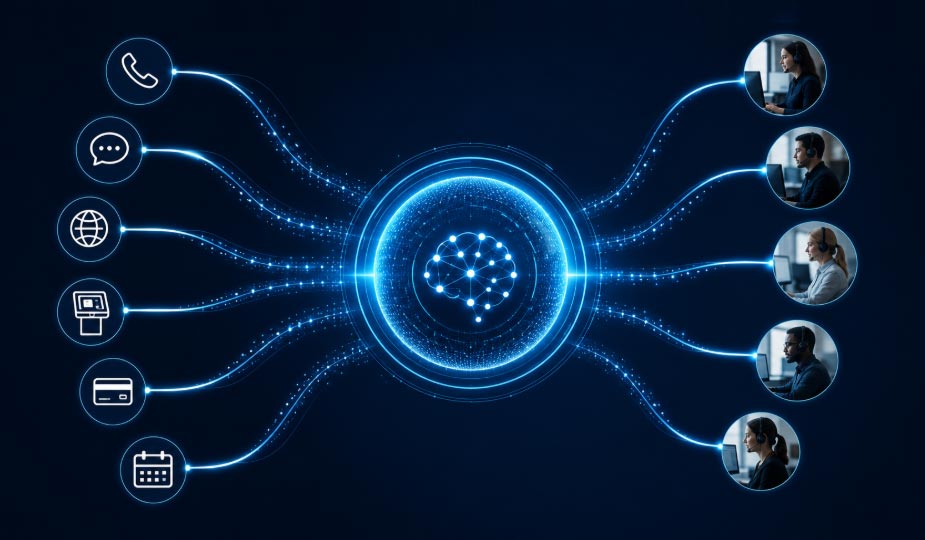
Figure 1. AI-enabled customer operations can unify calls, messaging, web inquiries, scheduling, payments, and routing into one intelligent operating layer.
Introduction
The front desk has always been more than a counter. In dentistry, medicine, wellness, hospitality, and other customer-facing environments, it is the first human touchpoint, the first operational filter, and often the first impression of the entire organization. A patient who is greeted with confidence feels safer. A customer whose question is answered quickly feels valued. A staff member who can rely on clear workflows has more time for the interactions that truly require judgment, empathy, and trust.
A new class of AI-enabled, human-like front-desk technologies is beginning to emerge. These systems may take the form of avatars, kiosks, volumetric displays, conversational agents, or holographic customer-service presences that sit at or near the reception area. In general terms, the purpose is not to remove the human element from the business. The more meaningful objective is to protect it: to allow staff to spend less time repeating routine instructions and more time providing thoughtful service where human involvement matters most.
From Reception Desk to Operating Layer
Traditional front desks are asked to manage an expanding range of tasks. They answer calls, greet visitors, schedule appointments, confirm information, route records, collect forms, explain policies, support payments, manage cancellations, respond to emails and messages, and calm frustrated customers. In many practices and businesses, this work is performed while the staff is simultaneously managing live patients, incoming calls, digital messages, and clinical or operational interruptions.
Human-like AI front-desk systems can transform this environment by becoming an operating layer rather than a simple screen. A well-designed system can greet a person, acknowledge arrival, guide check-in, support checkout, help direct forms, organize appointment requests, provide approved education, and route more sensitive issues to the appropriate team member. The result is not a colder experience; if designed correctly, it can make the front desk feel more responsive, more consistent, and more available.

Figure 2. A human-like front-desk presence can acknowledge patients, support the team, and create a more modern arrival experience.
Benefits Across the Customer Journey
The benefits of this emerging category are broad. First, these systems can help capture missed opportunities. Calls, texts, website forms, and after-hours inquiries often arrive when staff are unavailable or occupied. A front-desk AI presence can help capture intent, structure the request, and route the information so that the business can follow up instead of losing the opportunity.
Second, these systems can reduce front-office workload. Repetitive questions about hours, forms, directions, payment links, services, preparation, and scheduling can consume a large portion of staff time. When routine matters are handled consistently, staff can redirect attention toward relationship-based and judgment-based interactions.
Third, they can improve consistency. Different employees may explain policies, services, pricing pathways, preparation steps, or post-visit instructions differently. An approved AI workflow can deliver standardized language, reduce variation, and support a more predictable patient or customer experience.
A More Human Experience Through Better Workflow
The most interesting promise is not automation alone. It is the possibility of restoring a more human front-desk experience by removing avoidable friction. A patient who is immediately acknowledged does not feel invisible. A visitor who can complete forms privately feels more in control. A customer who receives a clear next step feels less uncertain. A staff member who receives organized information instead of scattered interruptions can respond with greater professionalism.
Touchscreen or private-screen options may also be important. Some matters should not be discussed loudly at a public counter. A private interaction path can help guide the person to a more discreet method of completing forms, reviewing general information, requesting staff support, or routing a question. This is especially relevant in healthcare-adjacent settings where privacy, dignity, and emotional sensitivity are central to the experience.

Figure 3. Holographic and avatar-based front-desk systems may support check-in, scheduling, communication, and workflow visibility.
Core Capabilities Likely to Define the Category
Although each product will differ, the category is likely to include a recognizable set of capabilities: greeting and recognition workflows, check-in support, checkout support, scheduling-request capture, billing and payment direction, call and message handling, email and phone inquiry routing, general service education, form guidance, document routing, multilingual support, customer follow-up, and staff escalation. Some systems may integrate through APIs with existing management software, scheduling tools, payment systems, communication platforms, or customer relationship systems, depending on availability, permissions, and configuration.
The more advanced systems may also become more useful over time. By reviewing recurring questions, common bottlenecks, repeated form issues, after-hours patterns, and escalation reasons, a business can refine approved workflows. In this supervised model, the system does not simply act on its own. It becomes more aligned with the business through controlled updates, approved scripts, and clearer routing rules.
Safety, Boundaries, and Professional Judgment
Healthcare and customer-service AI must be designed with boundaries. A front-desk system should not be presented as a clinician, lawyer, financial adviser, or substitute for professional judgment. Its role is best understood as administrative, educational, routing, and operational support. Sensitive, urgent, clinical, complaint-related, financial, uncertain, or out-of-scope matters should be escalated to designated human staff.
This boundary is not a weakness; it is one of the most important design features. The safest systems will be those that know when to stop, when to clarify, and when to involve a person. In healthcare, this distinction is essential. The front desk can be enhanced by AI, but trust still depends on appropriate human oversight, approved content, clear accountability, and careful workflow design.

Figure 4. Demonstration environments can help practices, business owners, and partners visualize the front desk as a more interactive operational platform.
Strategic Impact for Practices and Businesses
For dental offices, medical practices, med spas, wellness centers, hospitality organizations, and other service businesses, the front desk is becoming a strategic environment. It affects patient perception, customer retention, appointment flow, collections, reputation, staff morale, and revenue opportunity. A more responsive front desk can help a business feel larger, more organized, and more accessible without requiring every routine interaction to depend entirely on live staff capacity.
The potential benefits include missed-inquiry capture, faster response, 24/7 availability, front-office workload reduction, labor-pressure mitigation, staff-turnover resilience, consistent communication, improved first impressions, private document workflows, scheduling support, payment direction, billing and administrative routing, patient or customer education, human escalation, analytics, operational insight, multilingual access, private-label presentation, scalability across locations, and ongoing workflow optimization.
The next generation of front-desk technology should therefore be evaluated not by whether it looks impressive, but by whether it strengthens the core of the business. The best systems will not make customer service less human. They will help the human team become more present, more informed, and more available for the moments that matter.
Conclusion
Human-like holographic and AI-enabled front-desk systems represent a meaningful shift in how businesses may organize customer interaction. They are not merely futuristic displays. They are early expressions of a broader movement toward customer-facing operations platforms that combine presence, workflow, information, routing, and escalation.
If developed responsibly, these technologies may revolutionize the front desk by making it more responsive, more consistent, and more human-centered. The front desk of the future may not be defined by replacing people, but by giving people better support. It may be a place where technology greets, organizes, routes, and informs, while the human team remains available for empathy, judgment, and relationship. That balance is where the real revolution may occur.
Author Note: Dr. Kianor Shah is a dentist, lecturer, entrepreneur, and healthcare innovation strategist with interests in artificial intelligence, patient experience, implant dentistry, business operations, and the future of technology-enabled care delivery.
by top100admin | Jun 3, 2026 | AIMEDENT Journal Vol 1:3
Artificial Intelligence (AI) is rapidly reshaping dental practice as it is increasingly integrated into everyday clinical workflows. Avoidance of AI, whether due to hesitation or reluctance, is ultimately incompatible with successful practice. The underlying fear is that artificial intelligence may replace the clinician in the delivery of care; in reality AI functions as an advanced diagnostic adjunct, analogous to established technologies such as radiography, intraoral cameras, and cone-beam imaging.
Dentistry has traditionally relied on technical expertise guided by clinical judgment honed by years of training, with practitioners examining, diagnosing, and treating patients based on both evidence and experience. Artificial intelligence now supports a wide range of functions, including caries detection, periodontal assessment, radiographic interpretation, implant planning, and simulation of orthodontic outcomes. While these technologies do not replace clinical decision-making, they are exerting an increasingly significant influence in shaping it. Consequently, the clinician’s role is evolving from one centered primarily on procedural execution to one that emphasizes higher-level interpretation of complex data. The modern dentist functions as a decision-maker within a technologically augmented environment, where contextual understanding is as critical as technical execution.
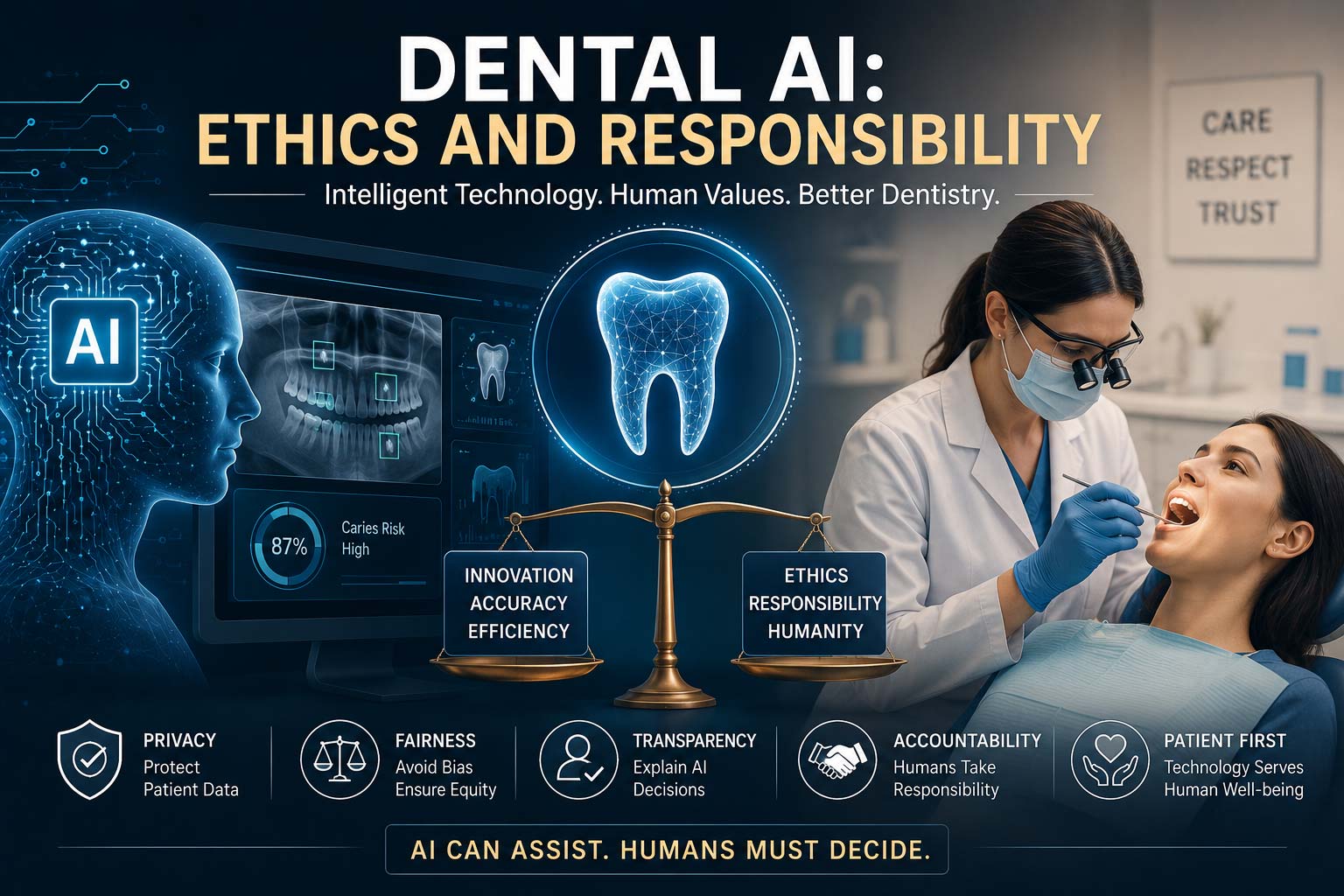
The integration of artificial intelligence introduces an additional layer of professional responsibility: the critical appraisal of algorithmic outputs. Clinicians must assess factors such as the quality and completeness of input data, the populations on which algorithms are trained, the potential for bias or uncertainty, and the extent to which AI-generated recommendations align with clinical findings. This expanded scope of judgment requires dentists not only to evaluate their patients but also to rigorously scrutinize the technologies informing their decisions. The clinician is the administrator and supervisor of both diagnostic processes and their supporting systems. These responsibilities must remain grounded in the core principles of medical ethics. Beneficence and non-maleficence require clinicians to prioritize patient welfare and to avoid harm, mandating critical engagement rather than passive acceptance of AI-derived recommendations. Respect for patient autonomy necessitates transparent communication regarding the role of AI in health care to support informed consent, while justice calls for the equitable and unbiased application of these technologies across patient populations.
Within this context, automation bias, the tendency to place undue trust in machine-generated outputs, emerges as a significant concern in AI-assisted healthcare. In dentistry, even subtle visual cues, such as AI-highlighted findings on radiographs, can influence clinical judgment, particularly under time constraints that may favor rapid acceptance over careful evaluation. Such reliance carries the risk of overtreatment, missed pathology, and diminished diagnostic scrutiny. Paradoxically, as AI systems continue to improve in accuracy, the potential for uncritical dependence may further increase.
The integration of artificial intelligence into healthcare underscores a fundamental ethical question: who bears responsibility for patient outcomes? Despite the growing role of AI, the clinician remains fully accountable for diagnosis, treatment planning, and clinical execution. Accordingly, AI should be regarded not as a substitute for clinical judgment, but as a tool to be applied thoughtfully, critically, and within established frameworks of professional responsibility.
Framing AI as a potential replacement for dentists is therefore misleading. The more substantive shift is one of transformation rather than substitution. AI is redefining, not diminishing, the clinician’s role, which increasingly centers on navigating complex, technology-enhanced decision-making environments where human judgment remains indispensable.
About the author
 George Freedman BSc, DDS, FIADFE, DiplABD, FAACD, FASDA, FPFA on behalf of the Artificial Intelligence Journal of Medicine and Dentistry (AIMEDENT Journal)
George Freedman BSc, DDS, FIADFE, DiplABD, FAACD, FASDA, FPFA on behalf of the Artificial Intelligence Journal of Medicine and Dentistry (AIMEDENT Journal)
georgefreedmandds@gmail.com
