Artificial intelligence has entered dentistry with remarkable speed. Machine learning systems now assist clinicians in detecting caries, interpreting radiographs, identifying periodontal changes, and screening oral lesions with levels of consistency approaching expert performance. Ethical discussion surrounding dental AI has largely focused on improving prediction accuracy. Clinical medicine recognizes uncertainty as an essential component of responsible diagnosis. This paper argues that responsible AI-assisted dentistry requires recognition of a critical ethical boundary — the moment at which automated diagnostic expression should be intentionally withheld.
Defining algorithmic silence
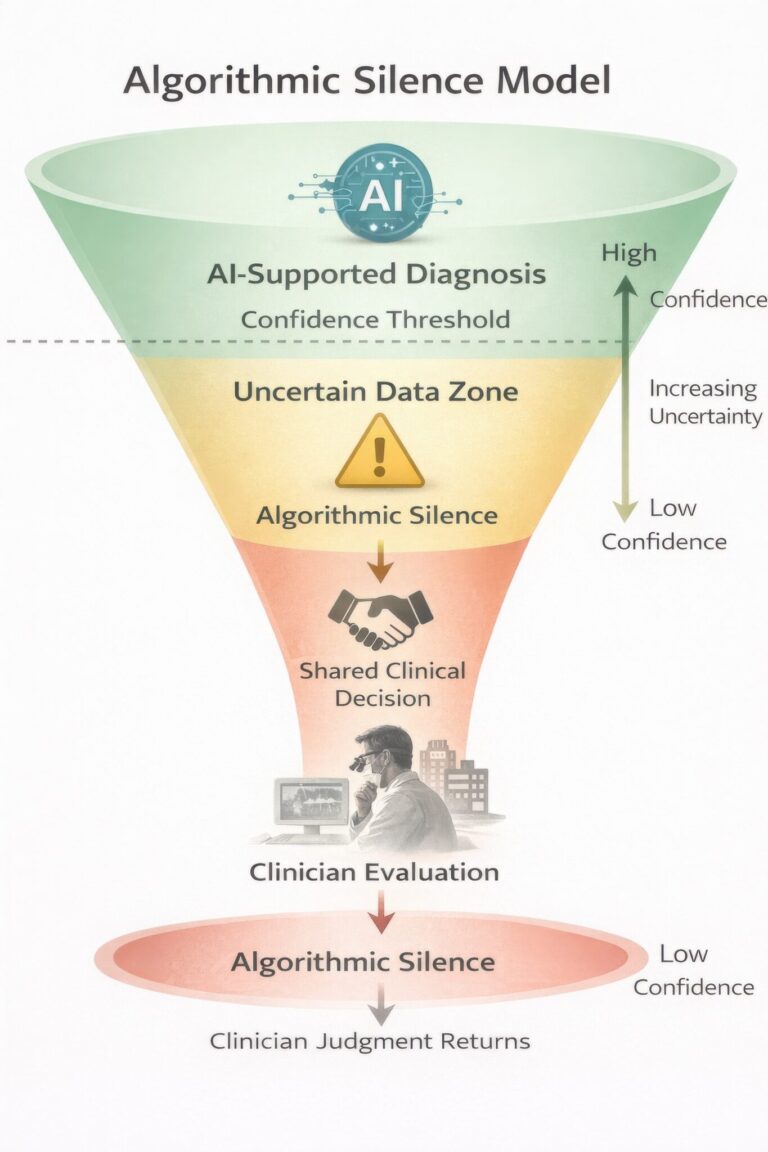
Algorithmic silence may be defined as the intentional withholding of automated diagnostic recommendation when model confidence, contextual validity, or ethical safety thresholds are not sufficiently satisfied. Silence functions as a designed safeguard embedded within clinical decision-support architecture, allowing uncertainty to become an actionable clinical signal.
Algorithmic silence in oral disease diagnosis
Oral disease diagnosis represents one of the most uncertainty-rich domains of healthcare. AI systems trained on image datasets may perform effectively in advanced disease detection while remaining vulnerable in early or atypical presentations. Calibrated abstention signals prompting referral or further investigation may better protect patients than forced classification.
Responsibility and clinical authority
Continuous algorithmic prediction introduces the risk of responsibility diffusion. Healthcare ethics maintains that the individual who decides bears responsibility. Algorithmic silence helps re-establish accountability by explicitly returning decision authority to the practitioner whenever uncertainty exceeds safe limits.
Algorithmic silence represents an essential evolution in AI-assisted oral healthcare. By embedding uncertainty awareness within clinical systems, dentistry can preserve professional judgment while benefiting from computational intelligence.
References
Amodei D, Olah C, Steinhardt J, et al. Concrete problems in AI safety. arXiv. 2016.
Kelly CJ, Karthikesalingam A, Suleyman M, Corrado G, King D. Key challenges for delivering clinical impact with artificial intelligence. BMC Medicine. 2019;17:195.
Schwendicke F, Samek W, Krois J. Artificial intelligence in dentistry: chances and challenges. Journal of Dental Research. 2020;99(7):769–774.
Floridi L, Cowls J, Beltrametti M, et al. AI4People—An ethical framework for a good AI society. Minds and Machines. 2018;28:689–707.
World Health Organization. Ethics and governance of artificial intelligence for health. Geneva: WHO; 2021.
European Commission. Artificial Intelligence Act. Brussels; 2024.
About the author
Dr. Ameed Khalid Abdul-Hamid is an Iraqi–British dental surgeon and academic researcher, internationally recognized for his contributions to artificial intelligence in dentistry and healthcare. He holds advanced qualifications from the University of Baghdad and the University of London, and is a Fellow of the Royal College of Surgeons (UK). Dr. Abdul-Hamid serves as Chairman of the Arab Organisation for Artificial Intelligence in Healthcare and Chairman of the Saudi-British Medical Forum (London). His research focuses on AI-enabled diagnostics, digital health systems, and the ethical, responsible integration of artificial intelligence in clinical care. In 2025, his work in dental artificial intelligence was published in the British Dental Journal, and he is a recipient of the Alan Turing Award in Dental Artificial Intelligence.
Clinical experience has limits, even in skilled hands. Clinical expertise remains a cornerstone of medical and dental practice. Years of training refine pattern recognition, inform diagnostic reasoning, and enable clinicians to navigate uncertainty in complex clinical environments. However, experience alone does not render clinicians immune to diagnostic error, particularly when disease presents with atypical features that fall outside classical descriptions. Diagnostic reasoning is also shaped by cognitive biases that can unconsciously influence clinical interpretation over time, potentially delaying more definitive investigation.
A routine referral that wasn’t routine
A 60-year-old male patient with a long-standing history of smoking was referred for what appeared to be a routine dental implant consultation. The referral did not raise immediate concern. However, clinical examination revealed a lesion on the lower lip that the patient reported had been appearing and resolving intermittently for nearly two years.
During that period, the patient had been assessed by both a medical doctor and a dentist. Because of its fluctuating presentation, the lesion was diagnosed as herpes simplex and managed conservatively. No biopsy was undertaken. Over time, the lesion persisted and increased in size, and the patient became increasingly self-conscious, even wearing a mask in public to conceal its appearance.
When a familiar diagnosis becomes a blind spot
On clinical assessment, the lesion’s characteristics were inconsistent with a benign viral condition. Its location, persistence, and the patient’s risk profile prompted urgent referral for biopsy. Histopathological analysis confirmed the diagnosis of lip melanoma, a rare but aggressive malignancy. The head and neck surgeon later indicated that had the diagnosis been further delayed by six to twelve months, the prognosis could have been significantly worse.
This case provides a clear example of anchoring bias, in which the initial diagnosis of herpes simplex influenced all subsequent clinical interpretations despite evolving evidence to the contrary. Anchoring bias is among the most frequently discussed cognitive biases in healthcare decision-making, affecting clinicians’ ability to revisit or revise diagnostic hypotheses when faced with new or discordant information.
Fig. 1
Pre-treatment
Pre-treatment
Fig. 2
Post-treatment
Post-treatment
Where AI could have changed the timeline
AI has the potential to intervene precisely at vulnerable points in the diagnostic process by providing objective pattern recognition that is independent of prior clinical assumptions. In dermatology and related domains, AI-based image analysis systems have demonstrated performance levels comparable to or exceeding those of experienced clinicians in detecting suspicious lesions when trained on large, well-curated datasets.
In this case, while AI would not replace histopathological diagnosis, the gold standard, it would have flagged the lesion as atypical and prompted earlier biopsy referral. This earlier flag might have reoriented clinical reasoning sooner, reducing a diagnostic delay.
Importantly, recent research shows that diversity and dataset quality are critical to AI performance: models trained predominantly on lighter skin tones may underperform on other populations, underscoring the need for equitable data representation.
AI as a clinical safety net
AI does not undermine clinical autonomy; instead, it serves as a safeguard against diagnostic inertia and cognitive blind spots. By introducing an objective analytical perspective, AI supports clinicians in identifying patterns that may be subtle or atypical, especially in early disease presentations or high-risk patient profiles. AI functions as a “second set of eyes,” complementing human judgment and prompting re-evaluation when visual or contextual features do not align with benign expectations. This aligns with broader evidence that AI systems can enhance lesion classification and risk stratification when integrated with clinical workflows.
Seeing risk before it becomes obvious
This case raises important questions for contemporary clinical practice. How many serious conditions are delayed because they resemble common, low-risk presentations? How often does initial diagnostic familiarity reduce ongoing vigilance? While early detection remains crucial for improving outcomes, early diagnostic doubt supported by objective tools like AI often makes timely intervention possible.
The future of healthcare will not be defined by clinicians or algorithms working in isolation. Human clinical reasoning, grounded in experience, context, and ethical judgment, must be augmented by AI’s capacity for large-scale pattern recognition and resistance to cognitive bias. Together, these strengths create a more resilient diagnostic framework.
In the case described, human clinical judgment ultimately altered the patient’s outcome. With AI integrated earlier into the diagnostic pathway, that judgment could have been supported much sooner.
References
Karimzadhagh, S., Ghodous, S., Robati, R. M., Abbaspour, E., Goldust, M., Zaresharifi, N., & Zaresharifi, S. (2026). Performance of Artificial Intelligence in Skin Cancer Detection: An Umbrella Review of Systematic Reviews and Meta‐Analyses. International Journal of Dermatology, 65(1), 69-85. doi: 10.1111/ijd.17981
Elumalai, K. (2024). Improving oral cancer diagnosis and management with artificial intelligence: A promising future for patient care. Oral Oncology Reports, 11, 100624. https://doi.org/10.1016/j.oor.2024.100624
Górecki, S., Tatka, A., & Brusey, J. (2025). Artificial Intelligence and New Technologies in Melanoma Diagnosis: A Narrative Review. Cancers, 17(24), 3896. doi: 10.3390/cancers17243896.
Ly, D. P., Shekelle, P. G., & Song, Z. (2023). Evidence for anchoring bias during physician decision-making. JAMA internal medicine, 183(8), 818-823. doi:10.1001/jamainternmed.2023.2366
Semerci, Z. M., Toru, H. S., Çobankent Aytekin, E., Tercanlı, H., Chiorean, D. M., Albayrak, Y., & Cotoi, O. S. (2024). The role of artificial intelligence in early diagnosis and molecular classification of head and neck skin cancers: a multidisciplinary approach. Diagnostics, 14(14):1477. https://doi.org/10.3390/diagnostics14141477
Papachristou, P., Söderholm, M., Pallon, J., Taloyan, M., Polesie, S., Paoli, J., … & Falk, M. (2024). Evaluation of an artificial intelligence-based decision support for the detection of cutaneous melanoma in primary care: a prospective real-life clinical trial. British Journal of Dermatology, 191(1), 125-133. https://doi.org/10.1093/bjd/ljae021
About the author
Dr. Shervin Molayem is a California-based periodontist and co-founder of Trust AI, the first AI-native patient management system in dentistry. He focuses on the oral-systemic connection, salivary diagnostics, and multimodal AI treatment planning. Dr. Molayem serves as a board member, advises, and invests in dental technology companies to accelerate innovation and modernize clinical care.
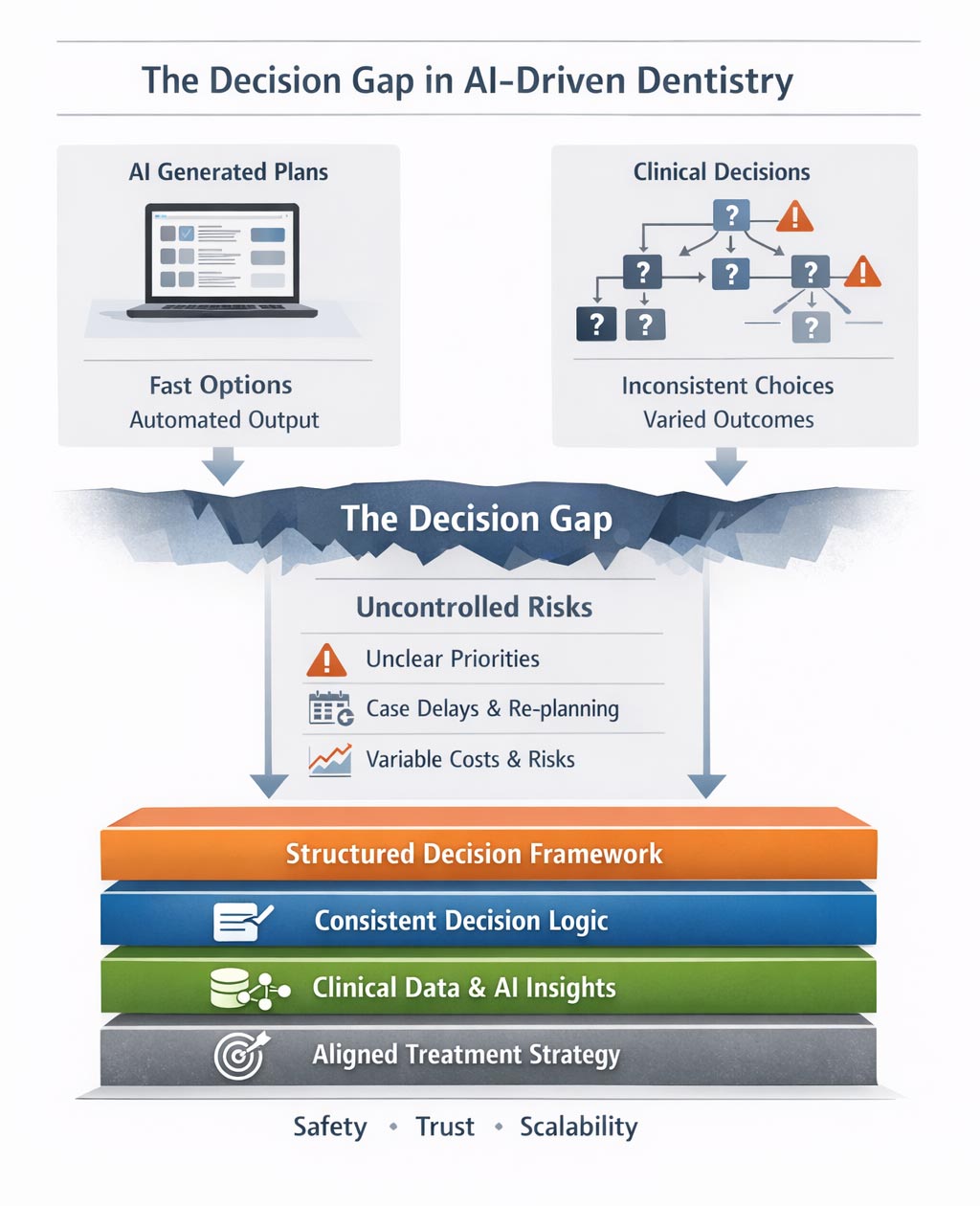
Why faster AI and prettier plans don’t solve inconsistency, risk, or scale in dental clinics
Over the past two years, artificial intelligence has moved rapidly into dental clinics. Treatment plans can now be generated in seconds. Clinical findings are converted into polished patient-facing PDFs. Documentation that once consumed chairside or after-hours time has become dramatically faster.
From a speed and presentation perspective, this is real progress.
Yet many clinic owners, operators, and senior clinicians are quietly reporting the same frustration: despite faster planning and better presentation, the underlying problems inside clinics haven’t disappeared.
Treatment plans are still inconsistent. Decisions still vary between clinicians. Cases still stall before treatment begins. And scaling beyond individual expertise remains difficult.
The issue is not that AI tools don’t work. The issue is that plan generation and clinical decision-making are not the same problem.
AI solved generation — not decisions
Most current AI systems in dentistry are excellent at generation. They summarize findings, propose options, and structure plans based on input data. They reduce manual effort and improve clarity compared to handwritten notes or fragmented documentation.
But generation answers a different question than the one clinics actually struggle with.
AI answers: “What could be done?”
Clinics struggle with: “Which option should we choose, why, and how do we remain consistent across cases and clinicians?”
That distinction matters more than it seems.
Generation ≠ decision-making
A treatment plan is not just a list of procedures.
It is a decision embedded in a broader context of: Risk tolerance
Clinical philosophy
Patient expectations
Long-term maintenance
Operational constraints
Legal and reputational exposure
Two clinicians can receive the same AI-generated plan and make different decisions about what to present, prioritize, or defer. Neither is necessarily wrong — but the clinic now carries variation that is rarely visible until something goes wrong.
AI tools do not resolve this variation.
They often amplify it, by producing plausible options without enforcing decision logic.
A clinic vignette: when AI makes inconsistency visible
Consider a multi-chair general practice that recently adopted an AI-assisted planning and presentation tool across all clinicians.
Within weeks, management noticed something unexpected.
Two patients with nearly identical profiles — moderate periodontal findings, early carious lesions, and signs of erosive wear — were seen by different clinicians. Both plans were generated using the same AI system. The layouts were clean. The language was professional.
The documentation looked standardized.
Yet the substance of the plans differed markedly.
One plan emphasized immediate periodontal stabilization and conservative monitoring. The other prioritized restorative treatment with a more aggressive intervention sequence.
Case acceptance, chairtime estimates, and projected costs varied significantly.
No clear clinical error was identified. Each plan could be defended.
What the AI exposed was not a software flaw — but the absence of a shared decision framework behind those choices.
Where inconsistency appears — before treatment even begins
Most treatment failures are not technical failures. They occur before treatment starts.
Clinic operators recognize these patterns immediately:
Cases accepted but never scheduled
Patients pausing due to unclear priorities
Replanning the same case multiple times
Internal disagreement on the “best” approach
Clinicians second-guessing their own recommendations
These are not problems of skill.
They are problems of decision coherence.
When decision-making remains implicit and experience-driven, clinics depend on personal authority rather than shared structure. That works at small scale — and quietly breaks as complexity increases.
Why operators and DSOs feel this first
Individual clinicians can often function comfortably with implicit reasoning. Operators cannot.
As clinics grow, operators face uncomfortable questions:
Why do similar cases produce different plans?
Why do some clinicians escalate risk faster than others?
Why does standardization feel restrictive rather than enabling?
Why does adding talent sometimes increase friction instead of performance?
These are not software problems. They are decision architecture problems.
AI makes planning faster, but it does not make reasoning visible, comparable, or repeatable.
The missing layer: decision consistency
Decision consistency does not mean uniform treatment. It means that differences are intentional, explainable, and defensible.
A consistent clinic can answer:
Why one option was chosen over alternatives
What risks were accepted or deferred
How a case aligns with clinic strategy
Where clinical judgment overrides automation
Without this structure, clinics rely on reassurance — not reasoning.
Polished PDFs may calm patients. AI-generated plans may look confident. But none of this guarantees that decisions are aligned, scalable, or safe over time.
From automation to accountability
Dentistry is entering a post-AI phase faster than many realize.
In this phase:
Plan generation is assumed
Speed is expected
Presentation is table stakes
The differentiator becomes how decisions are evaluated, compared, and repeated.
AI can generate options. Only structured reasoning creates accountability.
As regulatory scrutiny increases and clinics scale, the ability to explain why a decision was made will matter as much as what was done.
Decision consistency is not a luxury.
It is the infrastructure that allows AI to be used safely, intelligently, and at scale.
Closing thought
The question dentistry now faces is not: “How do we generate better treatment plans?”
But rather: “How do we make better decisions — consistently, defensibly, and at scale?”
AI solved one layer. The next bottleneck is already here.
About the author
Dr. Sami Savolainen is a dentist and healthcare systems thinker working at the intersection of clinical decision-making, documentation, and risk management. With experience in clinical practice and system design, he focuses on how planning structures determine safety, trust, and scalability in modern healthcare.
Everyone who has ever tried to introduce new technology into the practice of medicine knows how difficult this process is. The reasons are numerous, but the overarching issues are that patient safety is supremely important, and any new clinical tool must be vigorously tested to ensure its safety. Another issue is that the introduction of new tools into existing workflows has proven to be a complicated task that few wish to risk. These workflows have been developed over decades to be compliant with regulatory requirements, protect patient safety, and ensure care team collaboration and access. Introduction of new technology means disruption to these well-established workflows, potentially making the entire team’s life more difficult rather than easier.
It is interesting to note that technology helps automation in industries such as travel, hospitality, mobility, and more, but is less efficient in healthcare. One of the reasons is the fragmented nature of healthcare data, making automation of clinical, administrative or operational activities more difficult. While Amazon and Netflix can improve the consumer experience for shopping and streaming by having only a small slice of personal data in those areas, this is not possible in healthcare.
If a segment of the medical history is missing, decision-making support is not possible. Submitting a medical payment claim is unworkable if part of the patient’s work-up is not included in the documentation; insurance companies are always on the lookout for any reason to deny or reduce payment. Allowing AI to process and submit payment claims autonomously will simply not function if the radiology reporting system is not connected to the HER.
While progress has been made in interoperability, there are simply too many hubs to connect, even within a city, let alone in a state or a nation. Submitting a claim with prior authorization for a medication may not require full interoperability, but identifying health issues and gaps in care proactively, and addressing them effectively, requires near complete medical records. If a procedure was performed at one medical center, but the patient’s records at a different center do not show the results, it is a clear indication that neither center is fully aware of the patient’s health status, indicating a serious danger to the patient.
There is a perceived lack of clear evidence of clinical benefits or financial return on investment (ROI.) New technology requires the expenditure of money, time and effort. It must demonstrate some possible benefits, such as improving patient outcomes, enhancing clinical productivity, upgrading operational and administrative efficiency, increasing revenues, and/or lowering costs.
To show improved patient outcomes, you need to do real-world, prospective and controlled trials to document the promised benefits. Without that, you’re just making unsubstantiated claims, and the medical community is a tough crowd to do that to. They’ve shown to be quite uncooperative with anything that does not prove its claims through well-designed studies. A good example of this is all the various radiology AI solutions that read scans and “help” the radiologist with their workflows. All of them have FDA approval, a low bar that can be met by showing that your tool is as accurate as a radiologist in finding a defined abnormality. However, in most cases the studies show that using the AI in addition to the radiologist improves patient outcomes haven’t been done. What does that mean for those companies? Insurance companies are not paying for them and if patients want AI to assist the radiologist in reading their scans, they need to pay out of pocket. Most are opting not to, and these tools have seen limited adoption.
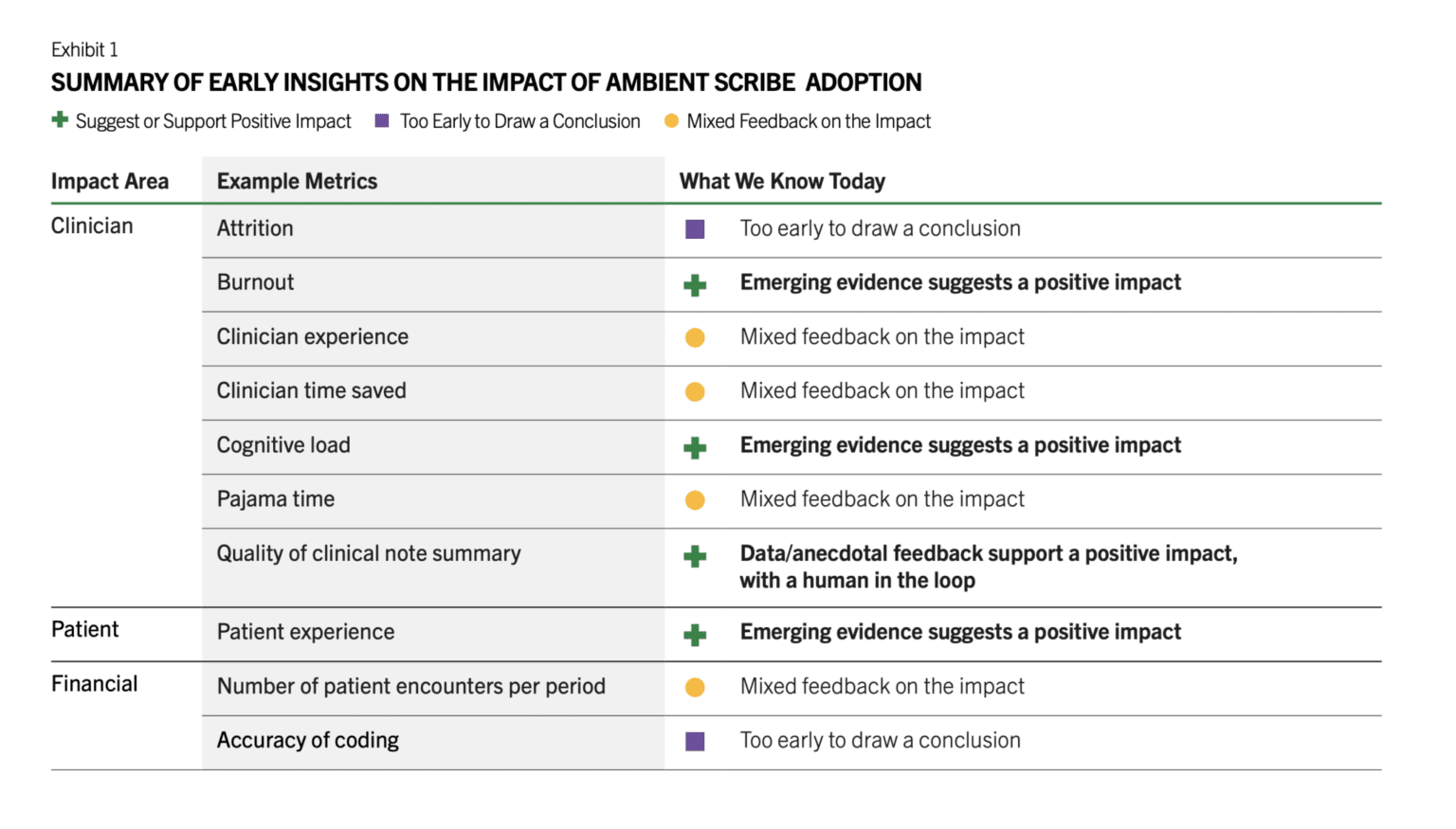
There are a number of other barriers such as the medical legal concerns by the providers, lack of the training of the staff in using them, lack of IT resources that can implement and monitor these tools, unclear regulatory framework, cost, and more. However, in the last 18 months, we have seen brisk adoption of some use cases such as ambient documentation, co-pilot function within the EHRs, and to a lesser extent autonomous coding. All of these are clinical workflow and administrative use cases. There is a reason for this. These are lower risk use cases that don’t involve clinical decisions, and none is fully autonomous. Doctors review the notes generated by ambient AI documentation tools and review any codes that are automatically created, and chart summaries are intended to save them time from reading a thick patient record but often that information is validated by the patient. It has been reported that the chart summaries contain numerous errors, necessitating physicians to review and verify the information, which reduces efficiency. There’s also emerging early evidence that there’s ROI for these tools. Peterson’s Health Technology Institute published a study that estimated lower burnout and cognitive load for physicians from the use of ambient AI documentation but the financial ROI to the health systems is not clear yet (Figure 1).
Source: Peterson Health Technology Institute
As for clinical AI tools, it doesn’t look like the studies needed are being done by companies and therefore adoption remains low. These studies take time and money, and most companies think they can magically drive adoption of their products without documenting clinical benefits. An RSNA study found that 81% of AI models dropped in performance when tested on external datasets. For nearly half, it was a noticeable drop, and for a quarter, it was significant. After these tools are approved, there’s no standard way to keep an eye on how they work across different scanners, hospitals or patient groups. In a recent interview with Health IT News, Pelu Tran, CEO and cofounder of Ferrum Health, opined that companies are not doing real-world studies to show that their tools perform as expected in that messy environment and that they result in improved patient outcomes. He calls for the buyers to demand solid evidence of clinical outcome improvement or financial ROI.
About the author
Dr. Ronald Razmi is the author of the “AI Doctor: The Rise of Artificial Intelligence in Healthcare” (Wiley, 2024) and former Cardiologist, McKinsey consultant, and CEO of digital health company, Acupera. He completed his medical training at the Mayo Clinic and holds an MBA from Northwestern University’s Kellogg School of Management.
The next wave of digital health—AI explainers, digital health avatars, and simulation-ready digital twins—will not thrive inside institution-tethered portals. These tools need comprehensive, longitudinal data assembled under a single, durable identity and governed by transparent, revocable consent. A patient-controlled personal health record (PHR) provides exactly that substrate. Recent federal policy has made consumer-mediated exchange both lawful and practical; meanwhile, advances in AI and FHIR standards make the PHR the most agile place to generate individualized guidance while protecting safety and privacy. Far from being a niche adjunct, a patient-owned PHR is the better platform for AI-directed care, patient engagement, and digital health equity.
Rails that finally favor the individual
The 21st Century Cures Act final rule prohibits information blocking and requires standardized, certified APIs that let patients access and use their electronic health information—cementing app-mediated retrieval as a baseline right.1 CMS’s Patient Access policies reinforce this architecture.2 Together they shift interoperability from institution-negotiated pipes to patient-authorized flows, enabling PHRs to aggregate data across sites, not just within a single portal.3,4,5,6 In parallel, TEFCA is standing up national exchange “rails.” Its Individual Access Services (IAS) pathway lets consumer apps retrieve a person’s records via QHIN networks—meaning a PHR can reach beyond one-off connections and into nationwide coverage. For older adults, Blue Button 2.0 adds multiple years of Medicare claims, essential for medication, risk, and adherence analytics that AI avatars will use.5
Why PHRs fit AI (and digital twins)
AI-directed tools need heterogeneous inputs: clinical records from multiple EHRs, claims, imaging, devices, and patient-reported outcomes. Portals are excellent for transactions (orders, messages) but remain siloed by enterprise. A PHR, by design, fuses cross-site data under a single, consented identity and can expose it—selectively—to analytic services that return lay explanations, adherence plans, and scenario-based simulations. The standards are ready: SMART/HL7 Bulk Data (Flat FHIR) supports cohort-level exports for quality and population health, while SMART on FHIR APIs handle patient-level access inside apps.7,8,9 These capabilities underpin both real-time coaching and “push-button population health.”1 For digital health twins, recent reviews highlight the need for rich, longitudinal, multi-modal inputs—a requirement a patient-controlled PHR can meet more readily than any single EHR portal or OS-tied aggregator.10
Safety and scope: clear lines for AI
The FDA’s final guidance on Clinical Decision Support (CDS) draws a workable boundary: clinician-facing software that merely supports decisions and allows the professional to independently review the basis qualifies as Non-Device CDS (i.e., outside device regulation).7 Patient-facing diagnostic, triage, or treatment claims, or analysis of signals/images, tip into SaMD and need clearance. This is ideal for PHRs: they can host patient-education AI (plain-language lab/imaging explanations, discharge checklists) and non-device CDS for clinicians today—while isolating higher-risk modules for separate FDA pathways tomorrow. That modularity is harder inside monolithic portals where features and claims blur across the product.7
Privacy that is strict—just different.
Many consumer PHRs operate outside HIPAA unless acting for a provider/plan; they are regulated by the FTC and a growing lattice of state health-data and biometric laws. The FTC’s modernized Health Breach Notification Rule (HBNR) explicitly covers health apps and connected devices and clarifies breach obligations.8 A PHR that bans ad-tech trackers on sensitive surfaces, uses purpose-specific, revocable consents, and maintains an auditable sharing ledger is not “unregulated”; it is accountable under a framework designed for consumer technologies. When a PHR contracts as a Business Associate (e.g., to document discharge teaching or write back to a chart), HIPAA simply governs those flows. This dual-regime architecture lets PHRs innovate quickly on consumer features while satisfying enterprise requirements when needed.
Engagement—and equity—are where PHRs shine.
If AI is to narrow disparities, it must meet people where they are: on mobile devices, after hours, and outside clinic walls. Pew Research reports that roughly nine in ten U.S. adults own a smartphone; mobile-only internet use remains common among lower-income populations—an adoption pattern tailor-made for a mobile-first PHR with plain-language explainers, SMS nudges, and proxy support for caregivers.11 Evidence already links digital engagement to operational gains: a systematic review finds patient portal use can improve outcomes and efficiency; other studies associate digital scheduling/portal use with fewer no-shows, a key lever for access in safety-net systems. A patient-controlled PHR generalizes those benefits across all sites of care rather than confining them to one portal.12 For population health, the same platform can consent patients into community and research initiatives, enabling culturally relevant education and data-donation models that include groups historically underrepresented in research—without sacrificing agency.
Better for payors, providers, and regulators
For payors, a member-authorized PHR provides fused clinical-plus-claims context to target outreach, support medication adherence, and close HEDIS/Stars gaps—without waiting for each provider’s portal to catch up. Blue Button 2.0 ensures that, at least for Medicare members, a robust longitudinal baseline is available on day one.2 For providers, a patient-owned longitudinal record reduces re-work (chasing CDs, re-taking histories), documents teach-back, and deflects routine “please explain my labs” messages by delivering explanations upstream—freeing clinical time for relationship-heavy tasks. For regulators, PHRs operationalize the intent of Cures and TEFCA: they convert “right of access” and “trusted exchange” into real-world, patient-directed data liquidity and inject competition at the edge, where innovation touches patients.1
What about the incumbents?
EHRs remain essential as transactional systems of record for orders, documentation, and revenue cycle. But they are ill-suited to be the only interface for AI-directed, patient-facing services. Their incentives are rightly aligned to clinician productivity and institutional compliance. A patient-controlled PHR occupies a different locus of control: it’s the individual’s canonical copy, portable across life contexts (new insurer, new employer, moving states), with consented APIs that let many AI services compete to deliver value. By design, that ecosystem is more modular: non-device education today; cleared SaMD add-ons tomorrow; Bulk Data for quality programs when a sponsor funds it; TEFCA IAS to fill any remaining connectivity gaps.6
A pragmatic way forward
Build to four near-term capabilities: (1) Cures-compliant FHIR connections for major portals, (2) Blue Button 2.0 for claims, (3) device/wearable feeds and patient-reported data, and (4) consented sharing with time-boxed, scope-limited links. Layer explainable AI that turns results into actions patients can take today; keep clinician-facing support transparent and reviewable to stay outside device scope; and reserve diagnostic/triage modules for separate SaMD tracks. Use Bulk Data exports, when authorized, to feed quality reporting and community programs. As TEFCA IAS matures, plug in to scale from regional to national without renegotiating one portal at a time.2
Conclusion
If we want AI avatars that actually help people, digital twins that simulate realistic trajectories, and engagement that narrows—not widens—disparities, we should stop forcing everything through institution-tethered portals. A patient-controlled PHR gives individuals total, auditable control of their health data; gives innovators permissioned access to the multi-modal fuel AI needs; and gives payors, providers, and regulators a scalable path to better outcomes with stronger accountability. With Cures, TEFCA, Blue Button, Bulk Data, and clear FDA/FTC guardrails, the policy and technical pieces are finally aligned. The most direct route to AI-directed health care that works for everyone—especially the underserved—is to put the patient-owned PHR at the center.
References
Office of the National Coordinator for Health IT. 21st Century Cures Act Final Rule (Interoperability & Information Blocking). 2020–2024. (Federal Register)
Mandl KD, et al. “Push-button population health: SMART/HL7 FHIR Bulk Data.” npj Digit Med. 2020. (PMC)
Katsoulakis E, et al. “Digital twins for health: a scoping review.” npj Digit Med. 2024. (Nature)
Pew Research Center. Americans’ Use of Mobile Technology and Home Broadband (2024). (Pew Research Center)
Carini E, et al. “Impact of patient portals on outcomes and efficiency: systematic review.” J Med Internet Res. 2021. (JMIR Publications)
About the author
Sanjaya Khanal, MD, FACC—Interventional cardiologist and Founder/CMO of MyMR, a patient-owned AI PHR. Harvard-trained, Associate Professor, IT director and Chief of Staff; med-device entrepreneur with multiple patents and publications advancing scalable, patient-centric care.


 Dr. Ameed Khalid Abdul-Hamid is an Iraqi–British dental surgeon and academic researcher, internationally recognized for his contributions to artificial intelligence in dentistry and healthcare. He holds advanced qualifications from the University of Baghdad and the University of London, and is a Fellow of the Royal College of Surgeons (UK). Dr. Abdul-Hamid serves as Chairman of the Arab Organisation for Artificial Intelligence in Healthcare and Chairman of the Saudi-British Medical Forum (London). His research focuses on AI-enabled diagnostics, digital health systems, and the ethical, responsible integration of artificial intelligence in clinical care. In 2025, his work in dental artificial intelligence was published in the British Dental Journal, and he is a recipient of the Alan Turing Award in Dental Artificial Intelligence.
Dr. Ameed Khalid Abdul-Hamid is an Iraqi–British dental surgeon and academic researcher, internationally recognized for his contributions to artificial intelligence in dentistry and healthcare. He holds advanced qualifications from the University of Baghdad and the University of London, and is a Fellow of the Royal College of Surgeons (UK). Dr. Abdul-Hamid serves as Chairman of the Arab Organisation for Artificial Intelligence in Healthcare and Chairman of the Saudi-British Medical Forum (London). His research focuses on AI-enabled diagnostics, digital health systems, and the ethical, responsible integration of artificial intelligence in clinical care. In 2025, his work in dental artificial intelligence was published in the British Dental Journal, and he is a recipient of the Alan Turing Award in Dental Artificial Intelligence.


 Dr. Shervin Molayem is a California-based periodontist and co-founder of Trust AI, the first AI-native patient management system in dentistry. He focuses on the oral-systemic connection, salivary diagnostics, and multimodal AI treatment planning. Dr. Molayem serves as a board member, advises, and invests in dental technology companies to accelerate innovation and modernize clinical care.
Dr. Shervin Molayem is a California-based periodontist and co-founder of Trust AI, the first AI-native patient management system in dentistry. He focuses on the oral-systemic connection, salivary diagnostics, and multimodal AI treatment planning. Dr. Molayem serves as a board member, advises, and invests in dental technology companies to accelerate innovation and modernize clinical care.
 Dr. Sami Savolainen is a dentist and healthcare systems thinker working at the intersection of clinical decision-making, documentation, and risk management. With experience in clinical practice and system design, he focuses on how planning structures determine safety, trust, and scalability in modern healthcare.
Dr. Sami Savolainen is a dentist and healthcare systems thinker working at the intersection of clinical decision-making, documentation, and risk management. With experience in clinical practice and system design, he focuses on how planning structures determine safety, trust, and scalability in modern healthcare.