Compare top rated health care attorneys in Miami on the Justia Lawyer Directory. View lawyer ratings, client reviews, awards, and case results, and schedule a consultation with a trusted local attorney.
For students interested in specializing in this area, we now offer an area of focus in health law. Students may fulfill the requirements for this area of focus through taking advantage of a number of exciting classes and experiential opportunities related to health law.
Artificial intelligence is everywhere today — woven into nearly every aspect of life and conversation. But what is it exactly, what can it do, and more importantly, how can it serve you and your patients?
To understand its role, we should start with definitions. “Artificial” refers to something made by humans rather than occurring naturally, often designed to simulate the real thing. “Intelligence” describes the capacity to learn, reason, adapt, and solve problems — abilities central to understanding and navigating the world. The term “artificial” sometimes carries negative undertones, suggesting something insincere or unnatural, while the word “Augmented” implies enhancement — making something more complete, effective, or capable.
“Artificial intelligence” (AI) is a branch of computer science devoted to developing systems that perform cognitive tasks typically requiring human intellect, such as learning, reasoning, and decision-making. These systems process data, identify patterns, and make predictions that often emulate human thought.
“Augmented intelligence” (AI), by contrast, is human-centric, focusing on collaboration between humans and machines. Instead of replacing human expertise, it enhances it — using advanced analytics and vast computational power to support better judgments and outcomes. In dentistry, this distinction is essential. Our profession thrives on human empathy, intuition, and ethical care. Therefore, dentistry should embrace an augmented, rather than purely artificial, approach — one that integrates machine learning and diagnostic data with the clinician’s judgment and compassion.
Yet this integration raises vital ethical questions. Borrowing inspiration from Isaac Asimov’s “Three Laws of Robotics,” we might propose similar principles for dental AI:
It must never harm a patient;
it must follow human direction within that constraint; and
it must protect its data integrity without violating the first two rules.
Augmented intelligence is a powerful addition to modern dentistry — one that, used ethically and wisely, will amplify human intelligence, empowering both practitioner and patient.
Sincerely,
George Freedman BSc, DDS, FIADFE, DiplABD, FAACD, FASDA, FPFA on behalf of the Artificial Intelligence Journal of Medicine and Dentistry (AIMEDENT Journal) georgefreedmandds@gmail.com
Documentation, attribution, and skepticism as clinical safety tools
Defensive medicine used to mean ordering one more test, writing one more line in the note, or documenting that risks were discussed “in detail.” That definition no longer holds. In the AI era, defensive medicine is less about doing more, and more about how decisions were made, who contributed to them, and how uncertainty was handled once artificial intelligence entered the workflow.
The medical record is no longer written by a single clinician at the end of a long shift. It is increasingly co-authored by ambient scribes, summarization engines, clinical decision support tools, and large language models that can sound confident even when they are wrong.
Here is the legal reality clinicians need to absorb early: When AI enters the chart, responsibility does not shift. It concentrates.
A shared workspace, personal liability
Most clinicians already use AI, whether they call it that or not. Ambient documentation, auto-generated assessments, triage tools, record summarization, and literature synthesis are now routine. These tools reduce friction and save time. But they also introduce a new medico-legal problem:
If an AI-generated statement is wrong and it appears in the chart, who owns it?
The law has been consistent so far. The signer owns the note. Courts do not meaningfully distinguish between human-authored and AI-assisted documentation. The medical record remains a clinician’s representation of reality, regardless of how the text was produced. That alone should change how we document.
Photo supplied
Hallucinations are a feature not a bug
They are the algorithm.
One of the most dangerous myths in healthcare AI is the belief that hallucinations are technical glitches that will be fixed with better models. They will not. Hallucinations are a structural feature of large language models. These systems do not retrieve truth. They generate statistically plausible language based on patterns in prior data. When ground truth is missing, incomplete, or outdated, the model interpolates. It fills in gaps. Fluently. Confidently.
This behaviour is not accidental. Models are rewarded for producing answers, not for saying “I don’t know.” In fact, any AI model that claims over 75 percent accuracy in a complex system shouldn’t be trusted. It’s probably learning the wrong thing very well.
Healthcare is a non-stationary system. Human behaviour changes. Policies shift. Clinical practice evolves. Data distributions drift. In such environments, extremely high accuracy often signals overfitting, false precision, or dataset leakage rather than real understanding.
Models can appear impressive by exploiting shortcuts:
Predicting the dominant outcome in imbalanced datasets
Learning documentation artifacts instead of physiology
Using correlation without causation
Performing well on historical data while failing quietly in real life
These are not bugs. They are the “cost of prediction” in living systems.
Language models amplify this risk. They sound authoritative. They write cleanly. They can fabricate references, guidelines, or reasoning unless the reader already knows the answer.
In healthcare, fluency without grounding is not neutral. It is dangerous.
Accuracy is not trustworthiness
We are repeatedly told to trust AI because it is “95 percent accurate.”
Accuracy is not safety.
Accuracy can hide bias.
Accuracy can ignore uncertainty.
Accuracy can collapse under distribution shifts.
In medicine, what matters is not how often a model is right in aggregate, but how it fails, when it fails, and whether humans can detect that failure in time.
Clean metrics do not equal resilient performance.
Photo supplied
“Who (or what) said what” now matters
This is where defensive medicine must evolve.
When AI contributes to clinical reasoning or documentation, attribution becomes a safety tool.
Compare:
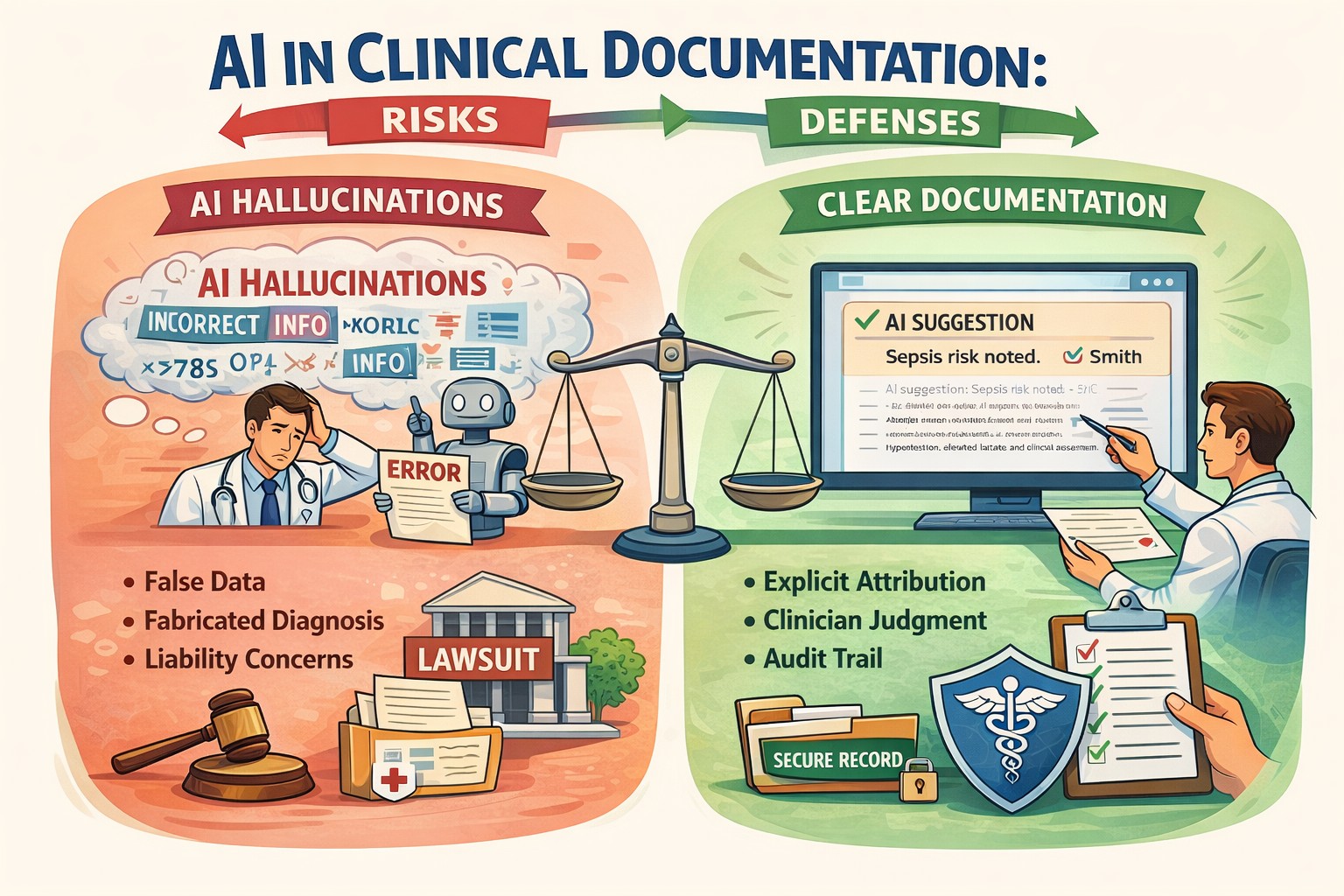
“Plan: initiate antibiotics due to concern for sepsis.”
with:
“AI-assisted decision support suggested possible sepsis; recommendation reviewed and accepted based on hypotension, lactate elevation, and clinical assessment.”
Clinically similar.
Legally and defensively, very different.
Attribution documents judgment. It shows that AI assisted but did not replace reasoning. Years later, that distinction can be very important.
The standard of care is already shifting
Rapidly and unevenly, AI is becoming embedded in expectations of care.
Radiology offers an early signal. In some settings, AI-assisted triage of brain imaging is routine. A future plaintiff may reasonably ask why available AI support was not used.
At the same time, clinicians may also be exposed when they use AI and override it, especially after adverse outcomes. This tension has been described as the negative outcome penalty paradox: clinicians can be punished whether they follow or reject AI recommendations once AI becomes normalized.
Defensive medicine now requires reasoned positioning, not blind adoption or avoidance.
Defensive documentation needs a major redesign
Traditional defensive documentation emphasized thoroughness.
Document when AI recommendations were rejected and why
Be cautious with AI-generated citations and guidelines
Preserve clinician reasoning, not just summaries
Several professional bodies and risk management groups now recommend transparency and disclosure around AI use in clinical documentation. This is not about longer notes. It is about defensible notes.
Training clinicians is now a legal issue, not just an educational one
One striking theme across medico-legal AI discussions is this: lack of AI literacy is becoming a liability risk. Using tools that you do not understand or failing to understand their limitations weakens your ability to defend your decisions.
Clinicians do not need to become data scientists. But they do need to understand:
What AI systems can and cannot do
Where hallucinations are most likely
How training data limitations affect output
Why confidence does not equal correctness
Ignorance will not be a defense when AI tools are widely available and increasingly normalized.
Augmented intelligence is the only defensible frame
Many organizations now favour the term augmented intelligence over artificial intelligence. That framing is crucial. Augmented intelligence keeps the clinician explicitly in the loop. It reinforces that AI assists but does not decide. The moment AI silently replaces reasoning in documentation, both patient safety and legal defensibility erode.
The chart is a legal narrative again
For years, clinicians were trained to treat notes as billing tools or handoff summaries. In the AI era, the chart reclaims its original role: a legal narrative of clinical reasoning under uncertainty.
AI can help write that story. It cannot own it.
Defensive medicine did not disappear in the age of AI. It matured.
About the author
Dr. Hassan Bencheqroun is a pulmonary and critical care physician, assistant professor at the University of California Riverside School of Medicine, and CEO of Medical AI Academy. He hosts “The AI-Ready Doctor podcast” and is an active AiMed participant and speaker bridging clinical care, education, and technology. He is actively focused on practical, clinician-safe AI adoption
The healthcare industry has entered a transformative era. Agentic artificial intelligence — systems capable of autonomous reasoning, planning, and multi-step task execution with defined human oversight — is transitioning from research concept to enterprise deployment. Unlike traditional machine learning that excels at narrow pattern recognition or generative AI that produces content reactively, agentic AI operates with goal-directed autonomy: decomposing complex objectives, coordinating specialized agents across disparate systems, and adapting strategies based on outcomes. This paradigm shift addresses healthcare’s most persistent challenges, including administrative burden consuming 20 percent of institutional budgets, physician burnout from documentation requirements, and the growing complexity of clinical decision-making.1
The acceleration in late 2025 has been remarkable. On December 1, 2025, the U.S. Food and Drug Administration announced agentic AI deployment for all agency employees — the first major regulatory body to institutionalize autonomous AI workflows for administrative functions including meeting management, document processing, and compliance operations.2 Critically, these internal tools support agency operations but do not autonomously render pre-market review decisions — human reviewers retain accountability for regulatory determinations. Days later, the Department of Health and Human Services released its comprehensive AI strategy positioning autonomous systems as central to federal health operations.3 For clinicians, administrators, patients, and healthcare entrepreneurs, understanding this transformation has become essential.
Defining the Agentic Paradigm
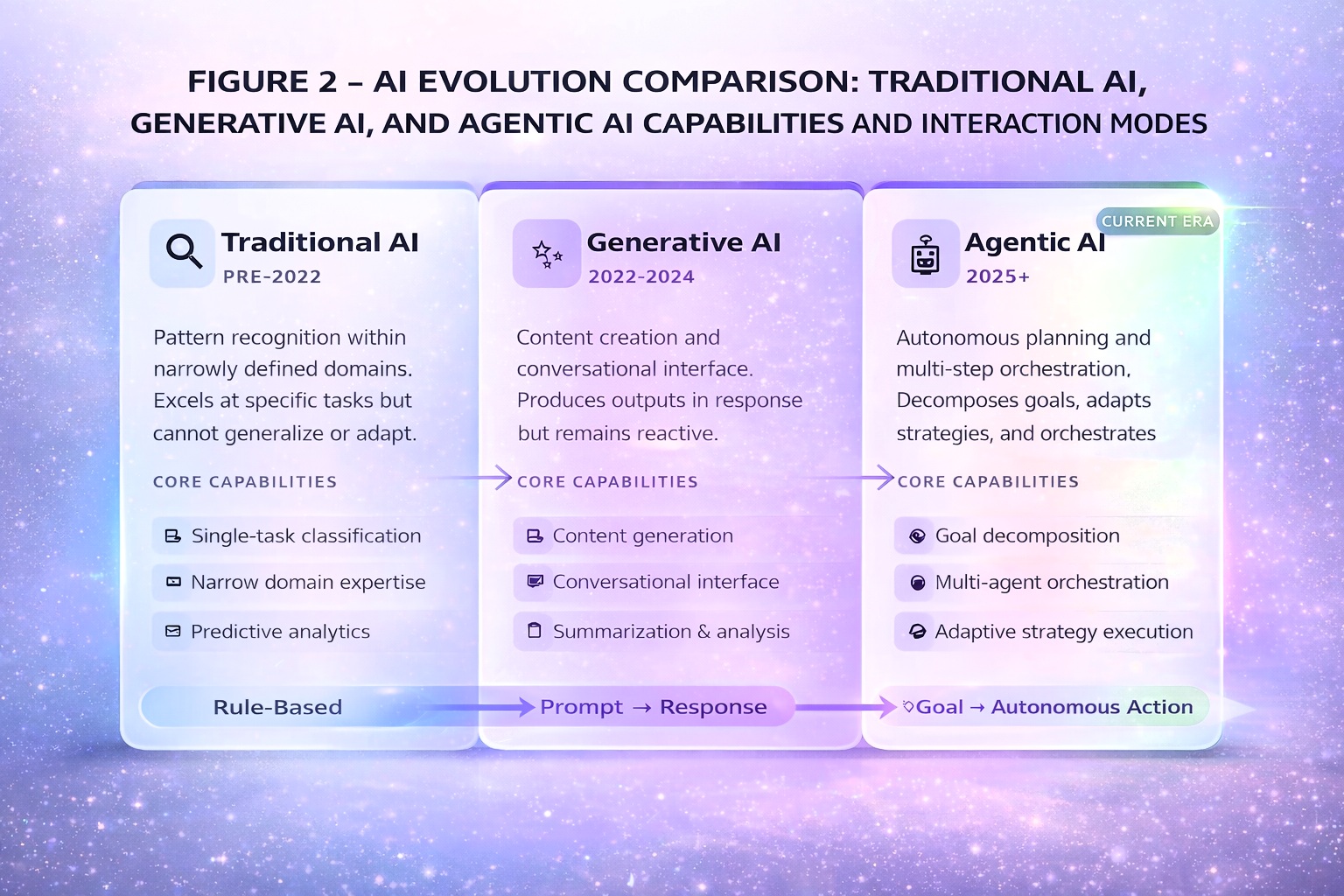
The distinction between agentic AI and its predecessors is substantive. Traditional machine learning excels at classification within narrow domains — identifying pathological findings in radiological images or predicting sepsis risk. Generative AI expanded to content creation and conversational interaction but remains fundamentally reactive. Agentic AI introduces systems that pursue defined goals with limited supervision, typically employing multiple specialized agents coordinated through an orchestration layer.4
Fig. 2
AI evolution comparison — Traditional AI, Generative AI, and Agentic AI capabilities and interaction modes
Technical precision requires distinguishing workflow automation from true goal-directed autonomy. Current enterprise deployments — Epic’s named agents, Microsoft’s orchestration framework — primarily automate predefined multi-step workflows with human checkpoints. Emerging research systems demonstrate more sophisticated autonomous reasoning, but these remain largely experimental. Research published in Frontiers in Artificial Intelligence found that agentic architectures can reduce cognitive workload by up to 52 percent compared to traditional clinical decision support, though this finding emerged from controlled simulation environments rather than clinical deployment.1 Healthcare leaders should maintain appropriate skepticism about vendor claims until validated outcome data emerges.
The enterprise technology landscape
The market is consolidating around major platforms. Microsoft’s healthcare agent orchestrator, unveiled at Build 2025, provides pre-configured agents with multi-agent orchestration for enterprise deployment, with pilot implementations at Stanford Medicine and Oxford University Hospitals.5 Epic Systems, serving approximately 38 percent of U.S. inpatient facilities with 325 million patient records, has deployed multiple AI agents: Emmie for patient engagement through MyChart, Art for provider communications, and Penny for revenue cycle management. However, access to these capabilities depends on Epic version, module licensing, and organizational readiness — many customers remain on versions predating agent functionality, and 6-12 months of configuration effort should be expected before realizing full value.6
Epic’s Cosmos AI foundation model initiative, trained on data from 275 million patients, may ultimately prove more transformative than individual named agents — representing a data advantage that competitors and startups cannot easily replicate. Nuance’s Dragon Copilot extends ambient documentation to nursing workflows, while the Atropos Evidence Agent proactively surfaces real-world evidence during clinical encounters without requiring explicit queries.7 For the 62 percent of hospitals not on Epic, integration complexity increases substantially, and Microsoft’s platform may offer broader interoperability.
Table 1: Healthcare Agentic AI Platform Comparison (January 2026)
Azure AI Foundry; broader EHR interoperability; piloting at academic centers
Epic (Emmie, Art, Penny, Cosmos)
Patient engagement, provider communications, revenue cycle, foundation model
Version-dependent; 6-12-month configuration; strongest for existing Epic customers
Nuance Dragon Copilot
Ambient clinical and nursing documentation, clinical query response
Generally available; multi-EHR integration; requires workflow design
Atropos Evidence Agent
Proactive real-world evidence delivery at point of care
Pilot deployments; addresses evidence accessibility gap
Regulatory landscape and liability considerations
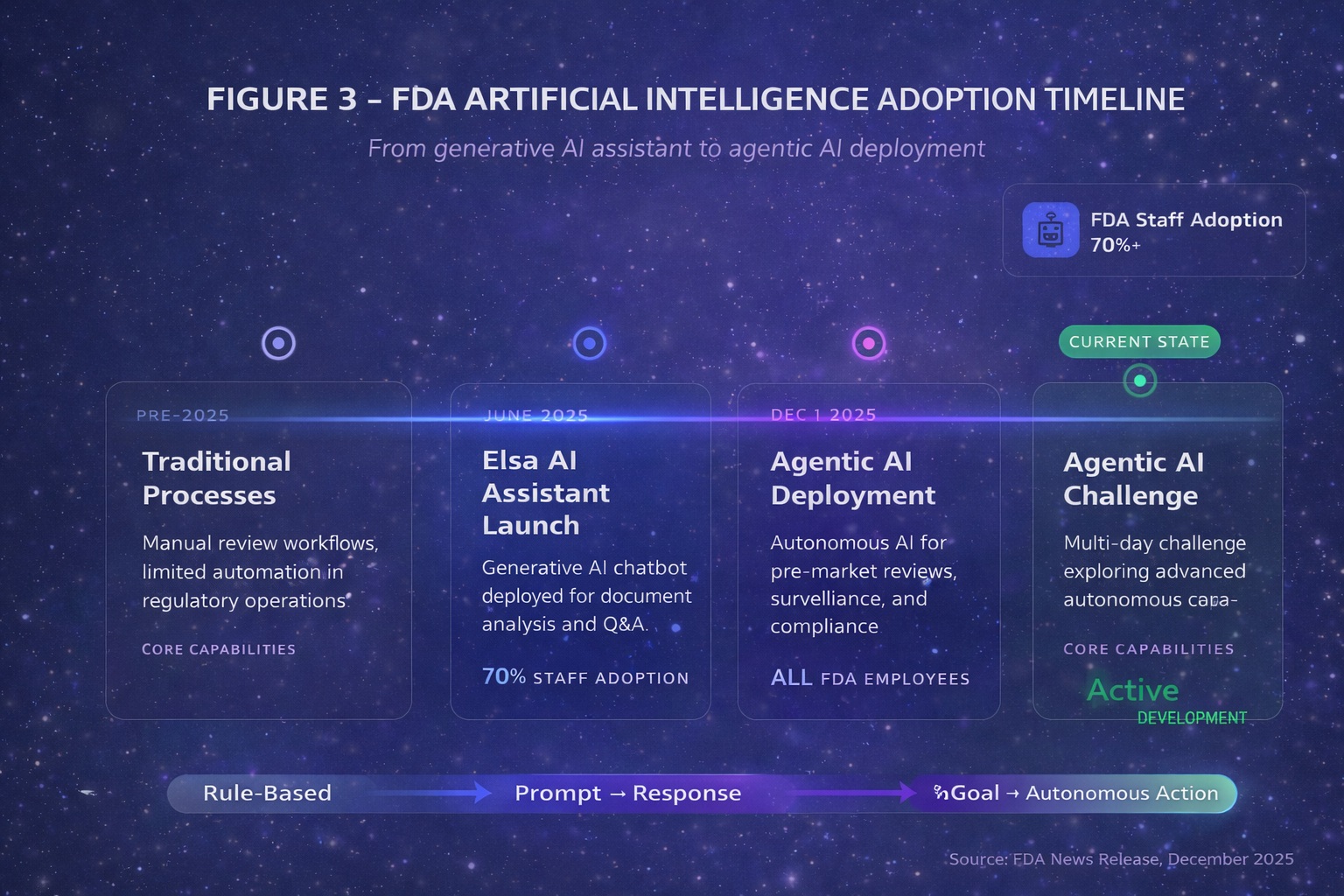
The FDA’s December 2025 agentic AI deployment requires careful interpretation. The agency’s autonomous systems support administrative functions within a secure GovCloud environment that does not train on industry submissions. This builds on the June 2025 launch of Elsa, a generative AI assistant now used by over 70 percent of FDA staff.8 The FDA’s database lists over 1,250 AI-enabled medical devices authorized for marketing, but the vast majority are narrow diagnostic imaging tools — not autonomous clinical agents. True agentic systems for clinical decision-making face the most stringent Class III regulatory pathway.9
Fig. 3
FDA AI adoption timeline – Elsa launch (June 2025) through Agentic AI deployment (December 2025)
International regulatory coordination is advancing. The European Medicines Agency and FDA jointly issued AI guidance for drug development, while EU Medical Device Regulation Article 14 mandates human oversight for high-risk AI systems — requirements that will significantly constrain autonomous deployment in European markets.10 State-level fragmentation compounds complexity: Illinois prohibits AI from making independent therapeutic decisions effective August 2025, Delaware is establishing an agentic AI regulatory sandbox, and Florida requires 24-hour written consent before AI records therapy sessions.11
The liability landscape presents novel challenges. The learned intermediary doctrine traditionally shields device manufacturers when physicians exercise independent judgment — but agentic systems that execute autonomously may eliminate the “learned intermediary”, exposing manufacturers to direct liability. When multi-step autonomous workflows result in patient harm, accountability allocation across vendors, health systems, and supervising clinicians involves unsettled legal questions. Organizations should demand clear contractual liability allocation and appropriate indemnification provisions before deployment.12
Patient safety and the automation challenge
Autonomous systems introduce safety considerations distinct from traditional clinical decision support. The patient safety literature documents automation complacency — the well-established tendency for humans to over-trust automated systems and fail to catch errors, a risk that increases with autonomy.13 Agentic systems may fail silently, with errors propagating through multi-step workflows before becoming clinically apparent. Healthcare organizations must conduct prospective hazard analysis before deployment, identifying anticipated failure modes and establishing detection mechanisms.
Current adverse event reporting infrastructure was designed for human and device errors, not algorithmic failures. Health systems deploying agentic AI should establish dedicated mechanisms for identifying, reporting, and analyzing AI-related safety events — including near-misses that existing frameworks may not capture. Governance architecture must include decision audit trails documenting agent actions, intervention protocols for human override, and continuous monitoring for emergent behaviors not apparent during validation.
The patient perspective deserves explicit attention. Early research on patient acceptance of AI-mediated care suggests significant variation based on task type, transparency, and perceived physician oversight. Patients generally accept AI for administrative functions and diagnostic support but express reservations about autonomous treatment decisions.14 Trust-building requires clear communication about when and how AI participates in care — something current disclosure frameworks inadequately address.
Workforce transformation and economic realities
Administrative tasks consume approximately 20 percent of healthcare institutional budgets, while physicians spend 13 percent of their time on similar responsibilities. Agentic AI targets precisely these activities.1 However, whether autonomous systems will substitute for clinical labour or complement it remains an open question with profound implications for workforce planning, medical education, and specialty choice. Research from Johns Hopkins identified a “competence penalty” whereby physicians using AI are perceived as less capable by peers and patients — creating adoption barriers even when AI demonstrably improves outcomes.15
Nursing workflows require particular attention. Nurses represent the largest clinical workforce and have distinct concerns about ambient AI documentation — including accuracy of captured information, workflow disruption during patient encounters, and implications for professional judgment. Dragon Copilot’s nursing extension requires careful workflow design and should not be deployed without nursing informatics involvement.
Economic analysis demands rigour beyond vendor projections. Implementation costs — including software licensing, integration, training, workflow redesign, governance infrastructure, and ongoing maintenance — are substantial. The productivity paradox, wherein IT investments historically fail to improve measured healthcare productivity, warrants appropriate skepticism.16 Reimbursement implications remain unclear: will payers reimburse for AI-augmented care, or will they demand discounts based on presumed efficiency gains? These dynamics will significantly influence adoption economics.
Strategic framework for healthcare organizations
Healthcare leaders face a fundamental build, buy, or partner decision. Organizations with substantial technical capacity and differentiated use cases may justify custom development. Most will purchase vendor solutions, with the critical choice being platform selection based on existing EHR infrastructure and integration requirements. Partnership models — embedding vendor capabilities within organizational workflows through co-development arrangements — offer middle-ground approaches.
Market trajectory data reinforces strategic urgency. While less than one percent of enterprise software incorporated agentic AI in 2024, Gartner projects 33 percent adoption by 2028, with the global market reaching $200 billion by 2034.17 Platform consolidation around Microsoft and Epic creates challenges for startups, though opportunities remain in vertical specialization, underserved care settings, and geographic niches where incumbents lack focus. Organizations developing institutional competencies now will establish advantages that later entrants cannot easily replicate.
The trajectory points beyond workflow efficiency toward fundamental care model transformation. When autonomous systems can conduct comprehensive health assessments in patients’ homes, when diagnostic capabilities requiring tertiary centres become available at community pharmacies, the very concept of a “medical visit” will evolve. Geographic distribution implications deserve attention: agentic AI may extend specialist reach to underserved areas where entire countries have only a handful of imaging experts, potentially democratizing access to clinical expertise.18
For healthcare leaders, entrepreneurs, and clinicians, the imperative is clear. Agentic AI is not a speculative future but an operational present reshaping regulatory process, clinical workflows, patient expectations, and competitive dynamics. Organizations that develop competencies in autonomous system governance, workforce adaptation, safety monitoring, and strategic deployment will capture the efficiency gains and quality improvements these technologies enable while managing the substantial risks they introduce. The transformation is underway. The strategic question is no longer whether to engage but how to lead — safely, ethically, and with appropriate humility about what remains unknown.
References
Hinostroza Fuentes N, Karim S, Tan L, AlDahoul N. AI with agency: A vision for adaptive, efficient, and ethical healthcare. Frontiers in Artificial Intelligence. 2025;8.
U.S. Food and Drug Administration. FDA Expands Artificial Intelligence Capabilities with Agentic AI Deployment. FDA News Release. December 1, 2025.
U.S. Department of Health and Human Services. HHS Artificial Intelligence Strategy. December 4, 2025.
IBM. What is Agentic AI? IBM Technology Documentation. 2025.
Microsoft. Healthcare Agent Orchestrator. Microsoft Build 2025 Announcement. May 2025.
Healthcare IT News. Epic unveils AI agents, showcases new foundational models at UGM 2025. 2025.
Microsoft Industry Blog. Agentic AI: Shaping the future of healthcare innovation. November 18, 2025.
Parenteral Drug Association. News Brief: FDA Expands AI with Agentic Deployment. December 2025.
Bipartisan Policy Center. FDA Oversight: Understanding the Regulation of Health AI Tools. November 10, 2025.
European Pharmaceutical Review. EMA and FDA issue joint AI guidance for medicine development. January 2026.
Manatt, Phelps & Phillips, LLP. Health AI Policy Tracker. 2025.
Price WN, Gerke S, Cohen IG. Potential liability for physicians using artificial intelligence. JAMA. 2019;322(18):1765-1766.
Parasuraman R, Manzey DH. Complacency and bias in human use of automation. Human Factors. 2010;52(3):381-410.
Longoni C, Bonezzi A, Morewedge CK. Resistance to medical artificial intelligence. Journal of Consumer Research. 2019;46(4):629-650.
Medical Economics. Physicians who use AI face a ‘competence penalty,’ Johns Hopkins study finds. 2025.
Himmelstein DU, Jun M, Busse R, et al. A comparison of hospital administrative costs in eight nations. Health Affairs. 2014;33(9):1586-1594.
Gartner. Top Strategic Technology Trends for 2025: Agentic AI. 2025.
Microsoft Research. The AI Revolution in Medicine, Revisited. Microsoft Research Podcast. July 23, 2025.
About the author
Dr. Srikanth Mahankali is a recognized authority in medical AI implementation and policy. As Chief Executive Officer of Shree Advisory & Consulting and a member of the NSF/MITRE AI Workforce Machine Learning Working Group, he has contributed to the development of national AI strategy while advancing responsible innovation in healthcare technology.

 George Freedman BSc, DDS, FIADFE, DiplABD, FAACD, FASDA, FPFA on behalf of the Artificial Intelligence Journal of Medicine and Dentistry (
George Freedman BSc, DDS, FIADFE, DiplABD, FAACD, FASDA, FPFA on behalf of the Artificial Intelligence Journal of Medicine and Dentistry (
 Dr. Hassan Bencheqroun is a pulmonary and critical care physician, assistant professor at the University of California Riverside School of Medicine, and CEO of Medical AI Academy. He hosts “The AI-Ready Doctor podcast” and is an active AiMed participant and speaker bridging clinical care, education, and technology. He is actively focused on practical, clinician-safe AI adoption
Dr. Hassan Bencheqroun is a pulmonary and critical care physician, assistant professor at the University of California Riverside School of Medicine, and CEO of Medical AI Academy. He hosts “The AI-Ready Doctor podcast” and is an active AiMed participant and speaker bridging clinical care, education, and technology. He is actively focused on practical, clinician-safe AI adoption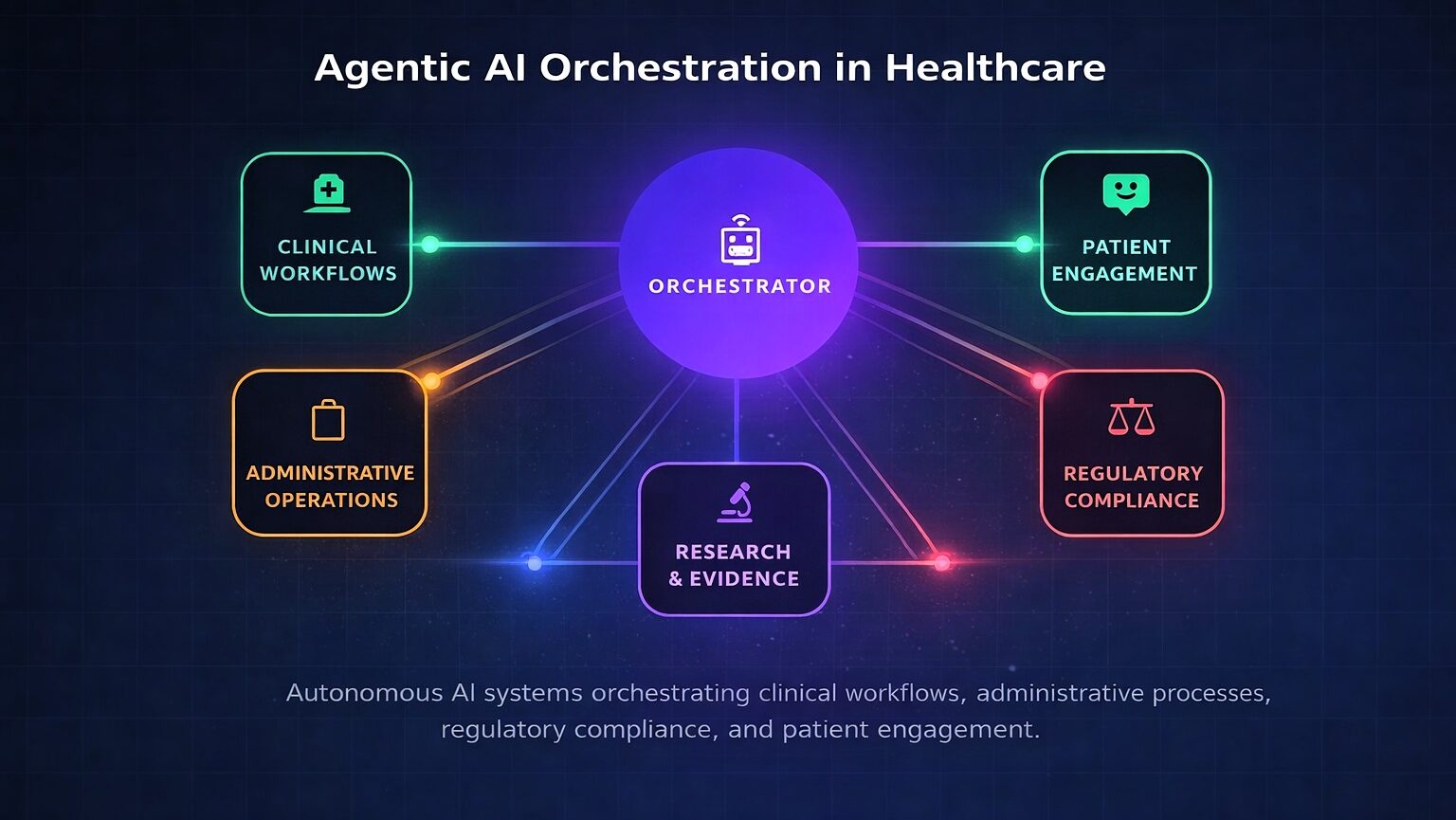
 Dr. Srikanth Mahankali is a recognized authority in medical AI implementation and policy. As Chief Executive Officer of Shree Advisory & Consulting and a member of the NSF/MITRE AI Workforce Machine Learning Working Group, he has contributed to the development of national AI strategy while advancing responsible innovation in healthcare technology.
Dr. Srikanth Mahankali is a recognized authority in medical AI implementation and policy. As Chief Executive Officer of Shree Advisory & Consulting and a member of the NSF/MITRE AI Workforce Machine Learning Working Group, he has contributed to the development of national AI strategy while advancing responsible innovation in healthcare technology.